2114
Reliability and accuracy of pediatric ventricular function analysis by short axis 'single-cycle-stack-advance' single-shot compressed sensing cines in minimal breath hold time1Royal Brompton Hospital, London, United Kingdom, 2Siemens Medical Systems, Erlangen, Germany
Synopsis
Cardiac cine SSFP by compressed sensing for ventricular volumetric analysis is promising for patients unable to tolerate long scanning sessions, as previously reported. We investigate a method requiring shorter breath-hold duration, robust to free-breathing if necessary, and assess its reliability and measurement accuracy for biventricular volume analysis in pediatric patients.
Introduction
Advances in cardiac cine SSFP by compressed sensing (CS) (1) for ventricular volumetric analysis are promising for patients unable to tolerate long scanning sessions, by enabling single breath-hold volumetric cine acquisition as previously reported (2,3,4). However, a long single breath-hold is required (eg for 10 slices, 20 cardiac cycles) which is sometimes impracticable; two cardiac cycles per cine slice are usually required, first for SSFP stabilisation and a second complete cycle is acquired for complete cardiac-cycle cine temporal coverage. While it is true that 3D whole-heart cine SSFP methods do not require that stabilisation cycle per slice, extra BH time is needed to sample the extended slab profile to avoid partition FOV wraparound effects. 3D is also intolerant of respiratory motion whereas we sought a reliable fast 2D multislice approach for clinical work. We therefore aimed to investigate a method requiring half the breath-hold duration and assess its reliability and measurement accuracy for biventricular volume analysis in pediatric patients, where unreliable breath-holding requires single-shot (“real-time”) cine imaging.Methods
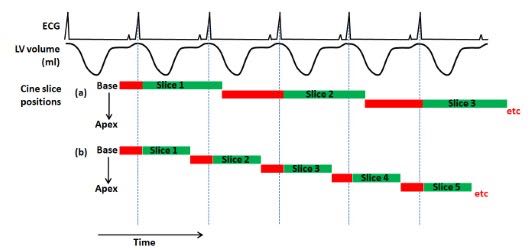
The compressed sensing cines were single-shot SSFP images as reported before (2-4). However, to halve the breath-hold time, we omitted SSFP stabilisation cardiac cycles before each SAX cine slice, accepting the associated limitation that the cines omit late diastole (Figure 1). Each prospectively-triggered cine captured from R-wave through systole to early diastole, when the sequence advanced automatically to the next SAX slice position to apply SSFP stabilisation before the next R-wave, titled "Single Cycle Stack Advance" (SCSA). The SCSA required only 1 RR interval per slice, considered potentially more realistic in pediatric patients than the doubled breath-hold of retrospective cines explained above. All cines in this work were 8mm SLT with 2mm gaps, with approximately matched acquired temporal and spatial resolutions.
We enrolled 27 consecutive pediatric patients (aged 13.1±2.8 years; 14 with congenital heart disease, 13 cardiomyopathy) (SIEMENS 1.5T SQ-engine VE11C, standard cardiac array receiver coils). Conventional multiple breath-hold cine SSFP stacks acquired for clinical work in the same scanning session were taken as “gold-standard” reference for comparison. End-diastolic measurement of each slice was obtained at the R-wave, circumventing the shortcoming that the prospective cine acquisition omits late diastole. Volumetric analysis was performed for SCSA and conventional stacks using CVI 42 software by a single experienced reader.
Results
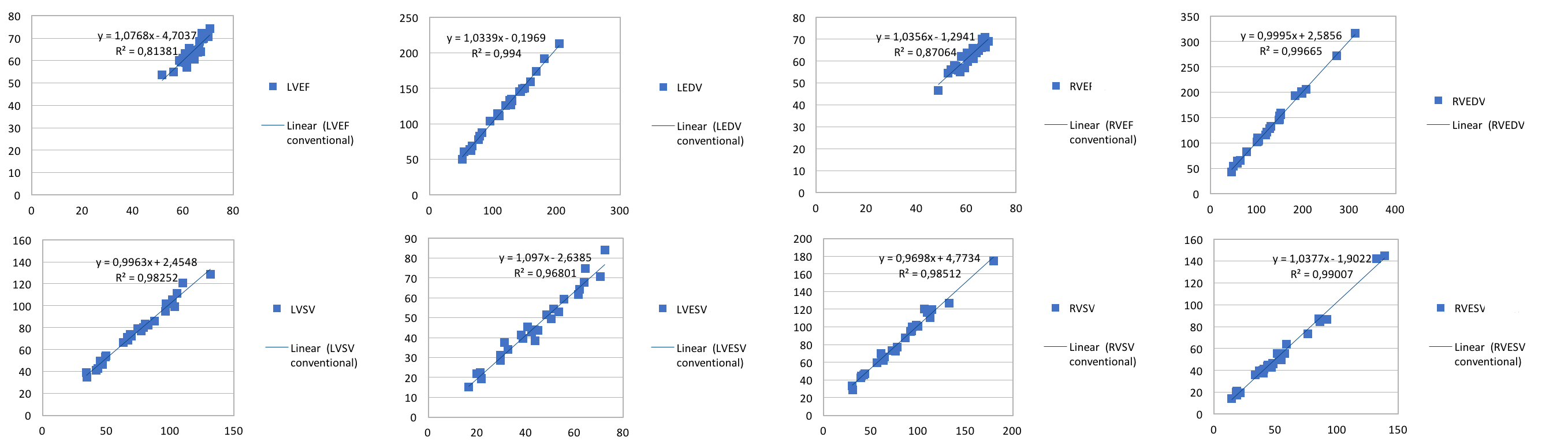
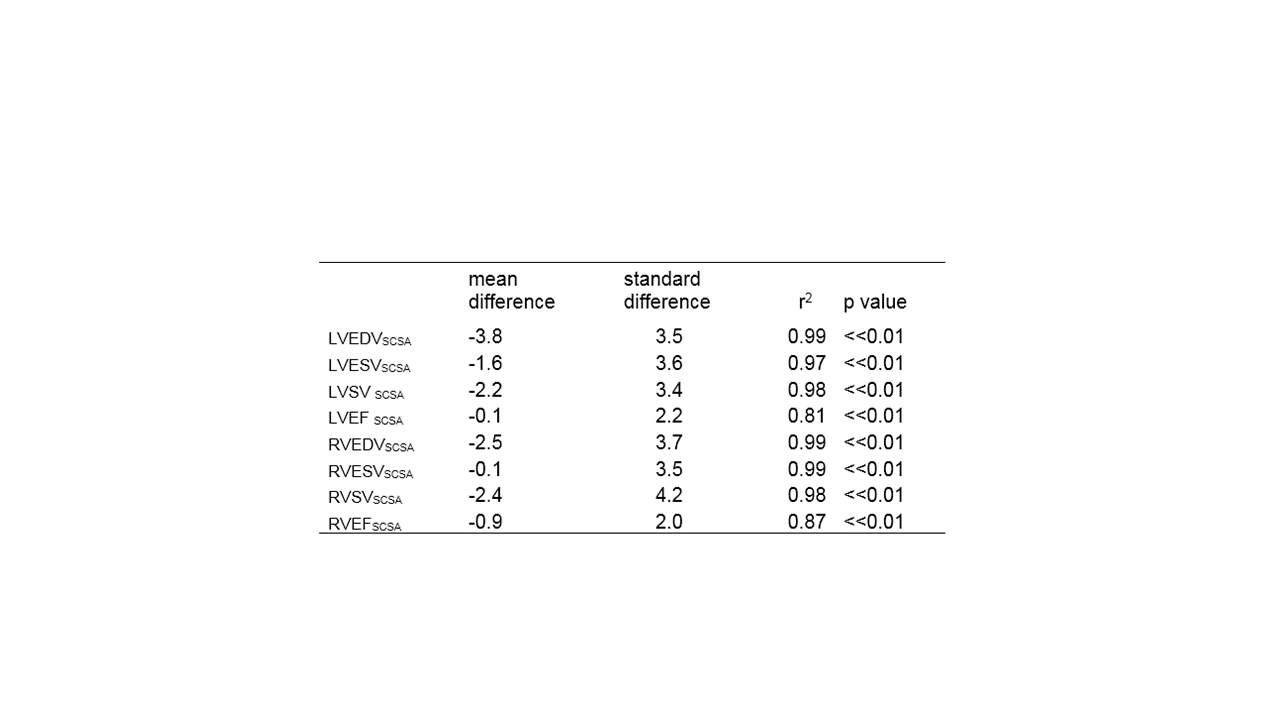
Linear regression analysis showed lower biventricular volumes and ejection fraction values for SCSA method but the difference from conventional was not significant (Table 1). The correlation between two methods was strong for all the directly measured ventricular parameters (LVEDV r2 0.99 p<0.01, LVESV r2 0.97 p<0.01, RVEDV r2 0.99 p<0.01 and RVESV r2 0.99 p<0.01), and slightly weaker for the derived parameters such as LVEF and RVEF (Figure 2).Discussion
Potential end diastolic volume underestimation by SCSA (2) was small, perhaps because the first frame 29ms after R-wave triggering was sufficiently prompt on this version of hardware and software, although that is often not the case. Poor ECG quality and misidentification of other ECG waves (such as MHD artefact) for triggering could potentially delay the first frame. SSFP stabilisation artefacts were not apparent on the first SCSA cine frames, for several reasons: 1. as shown on Figure 1, in SCSA there was usually some SSFP stabilisation in the late-diastolic phase of the previous cycle; 2. a cardiac shim was mandated for SCSA to minimise unnecessary off-resonance errors; 3. this work was at 1.5T not 3T, and 4. it is possible that the shorter T1 post-contrast agent (GBCA) might shorten SSFP stabilisation times; however, this was not a necessary requirement of the SCSA method; simply for clinical 'workflow' reasons, all ventricular volumetry cines were acquired post-GBCA, and GBCA was given for clinical purposes in the majority of these patients.
Although single-shot imaging is robust during free-breathing, that complicates comparing against the gold-standard breath-hold cines for ventricular analyses; therefore, for this work patients usually performed the short breath-hold for the CS cine stack. Some trade-off in CS diagnostic image quality was noted, but it reduces multiple breath-holds required from children, and overcomes interslice misalignment by inconsistent breath-hold positioning in the conventional cine stack.
Conclusion
All left and right ventricular parameters measured by SCSA acquisition in this pediatric patient population adequately correlated with conventional cines. The SCSA approach halves the single breath-hold duration, while underestimation of ventricular parameters is not statistically significant.Acknowledgements
No acknowledgement found.References
1. Gamper U, et al. Compressed Sensing in Dynamic MRI. Magnetic Resonance in Medicine 59:365–373 (2008)
2. Kido T, et al. Compressed sensing real-time cine cardiovascular magnetic resonance: accurate assessment of left ventricular function in a singlebreath- hold. Journal of Cardiovascular Magnetic Resonance (2016) 18:50
3. Vincenti G, et al. Compressed sensing single-breath-hold CMR for fast quantification of LV function, volumes, and mass. JACC Cardiovasc Imaging 2014;7:882–92.
4. Feng L, et al. Highly accelerated real-time cardiac cine MRI using k-t SPARSE-SENSE. Magn Reson Med. 2013 Jul;70(1):64-74.
Figures