2112
Left ventricular longitudinal contribution to stroke volume in pregnancy complicated by preeclampsia and normal pregnancy compared to non-pregnant controls1Clinical Physiology, Department of Clinical Sciences, Lund University, Skane University Hospital, Lund, Sweden, 2Physiotherapy, Department of Health Sciences, Lund University, Lund, Sweden, 3Obstetrics and Gynaecology, Department of Clinical Sciences, Lund University, Skane University Hospital, Lund, Sweden, 4Diagnostic Radiology, Department of Clinical Sciences, Lund University, Skane University Hospital, Lund, Sweden
Synopsis
We hypothesized that cardiac pumping in healthy pregnancy and pregnancy complicated by preeclampsia would be affected by the increased volume load on the heart during normal pregnancy and increased pressure load in pregnancy complicated by preeclampsia. The aim of this study was therefore to compare healthy pregnant women and women with preclampsia to healthy non-pregnant controls matched for age and cardiac index. The results were unexpected. Women with preeclampsia did not differ compared to healthy non-pregnant controls, whereas healthy pregnant women had significantly lower atrioventricular plane displacement and consequently a lower longitudinal contribution to stroke volume.
Background
During healthy pregnancy, cardiac output increases by up to 45%, primarily during the first trimester1. Thus the left ventricle is exposed to a significantly increased volume load during almost 40 weeks. About 3-6% of pregnancies are complicated by preeclampsia, a life threatening condition characterized by general endothelial damage causing vasoconstriction, hemoconcentration, edema and proteinuria, all manifests occurring after 20 weeks of gestation in formerly normotensive women. As shown by Simmons et al.2, women with preeclampsia have significantly higher systemic vascular resistance, however due to endothelial leakage lower blood volume. Thus, in women with preeclampsia the left ventricle is exposed to an increased pressure load at a normal volume load. Cardiac pumping mechanics can be divided into a longitudinal and a radial component, where the longitudinal pumping previously has been shown to contribute to 60% of left ventricular stroke volume3. The aim of this study was to investigate how left ventricular pumping mechanics adapt to normal pregnancy (volume load) and pregnancy complicated by preeclampsia (pressure load) by determining the left ventricular longitudinal contribution to stroke volume and to compare this contribution in pregnant women to matched non-pregnant controls.Methods
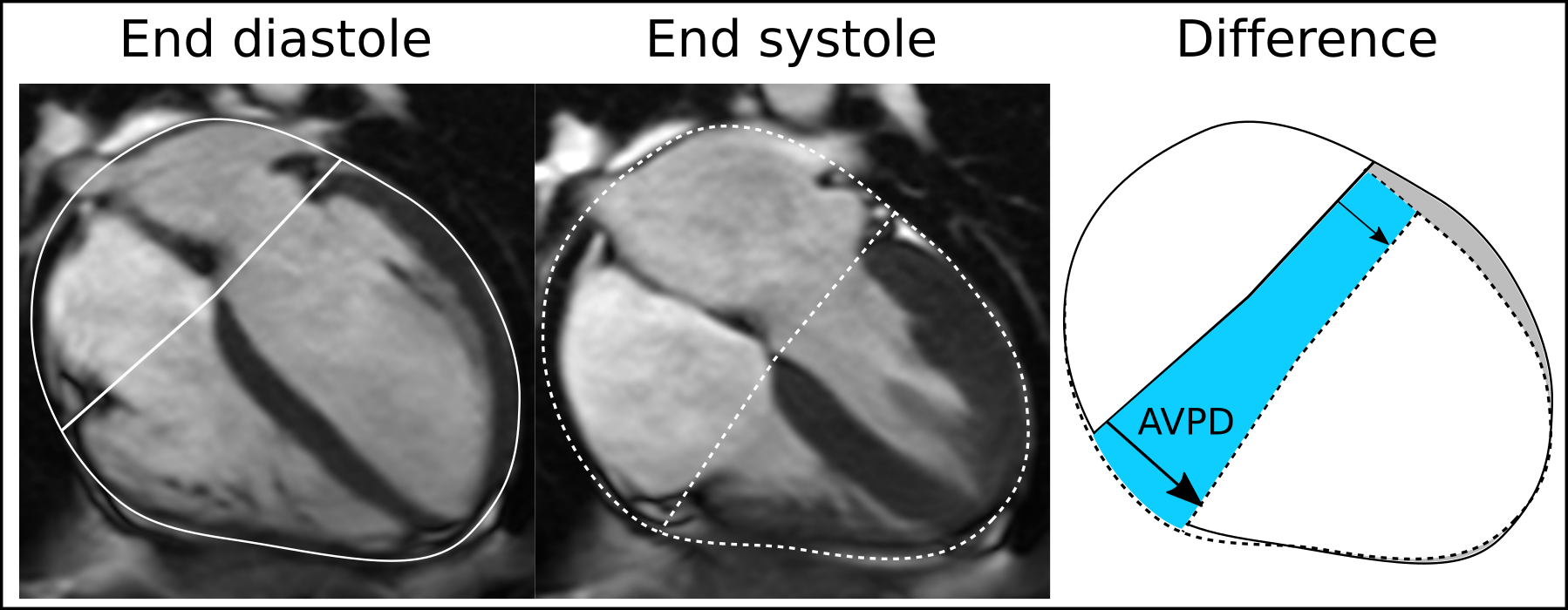
The Regional Ethical Review Board approved the study and all participants signed informed consent. Ten women with normal pregnancy (30±6 years; gestational week 36 (33-39)) and seven women diagnosed with preeclampsia (31±7 years; gestational week 31 (26-35)) underwent cardiovascular magnetic resonance (CMR) imaging during their third trimester. Twelve non-pregnant controls (30±6 years) matched for cardiac index and age were retrospectively included from a previous study. Imaging was performed on a 1.5T Siemens Aera or a 1.5T Philips Achieva using phased-array coils. All pregnant women were imaged in the left lateral decubitus position to prevent the fetus from compressing the inferior vena cava and thus affecting venous return and ventricular volumes. Non-pregnant controls were imaged in the supine position. Short-axis cine images covering the ventricle and long-axis images in the 2-, 3- and 4-chamber views were acquired using a standard balanced steady-state free precession (bSSFP) sequence with typical parameters 1.3×1.3×8mm3, TR/TE=3/1.4 ms, flip angle=60° and 30 time phases per cardiac cycle. Longitudinal contribution to stroke volume was calculated as the displacement of the atrioventricular plane multiplied by the short axis area3 (Figure 1). Left ventricular stroke volume was measured using planimetry. Statistical analysis was performed using Kruskal-Wallis non-parametric test with Dunn’s post-hoc correction.Results
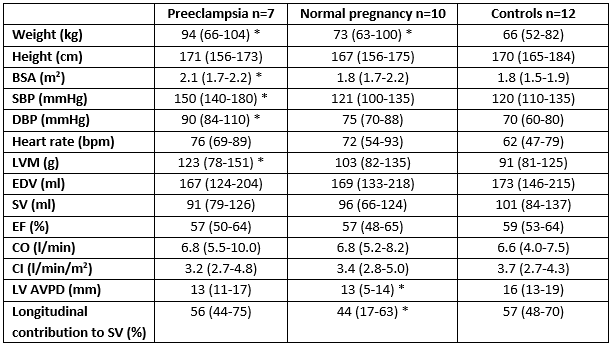
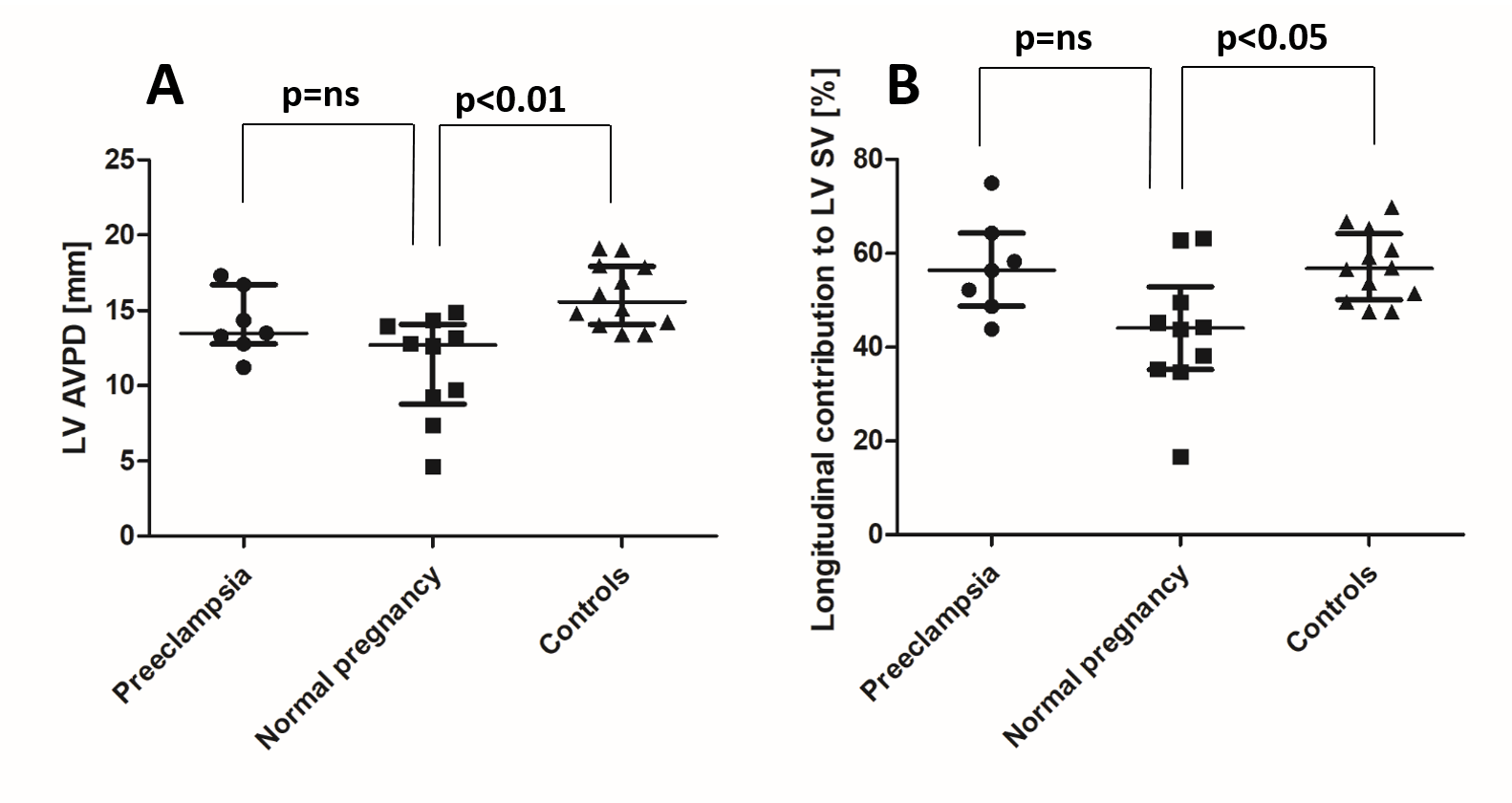
Subject characteristics and measures of left ventricular volumes and mass are presented in Table 1. Left ventricular atrioventricular plane displacement (AVPD) was 13 mm (range 11-17) in preeclampsia, 13 mm (range 5-14) in normal pregnancy and 16 mm (range 13-19) in non-pregnant controls (Figure 2, Panel A). Left ventricular longitudinal contribution to stroke volume was 56% (range 44-75) in preeclampsia, 44% (range 17-63) in normal pregnancy and 57% (range 48-70) in non-pregnant controls (Figure 2, Panel B).Discussion
The findings of the present study were unexpected. The heart is a pump where the right side is often referred to as a volume pump, pumping large volumes of blood against a low pressure. Therefore longitudinal pumping is more pronounced for the right ventricle and contributes to 80% of stroke volume. In contrast, the left ventricle is a volume and pressure pump, pumping the same blood volume but against a higher pressure. Thus the left ventricle is more dependent on the radial squeezing motion of the myocardium and longitudinal pumping instead only contributes to 60% of stroke volume. Based on the physiology and pathophysiology in the present study population, an increased longitudinal contribution to stroke volume in women with normal pregnancy would have been expected as these women have a larger volume to deliver at a normal pressure. In contrast, women with preeclampsia were expected to have decreased longitudinal pumping and thus be more dependent on radial motion of the ventricle in order to overcome the increased pressure load. Future work within this project involves studying the right ventricle to further increase our understanding of cardiac pumping during normal pregnancy and pregnancy complicated by preeclampsia.Conclusion
In the present study, there was no difference in longitudinal pumping between women with preeclampsia and non-pregnant controls. Interestingly, normal pregnancy was shown to have a lower longitudinal contribution to stroke volume compared to both women with preeclampsia and non-pregnant controls. These findings combined with further analysis of the data will lead to new physiological insights about cardiovascular adaptations to normal as well as complicated pregnancies.Acknowledgements
No acknowledgement found.References
1. Boron WF, Boulpaep EL. Medical physiology. Philadelphia, PA: Elsevier; 2016.
2. Simmons LA, Gillin AG, Jeremy RW. Structural and functional changes in left ventricle during normotensive and preeclamptic pregnancy. American journal of physiology Heart and circulatory physiology. 2002;283(4):H1627-33.
3. Carlsson M, Ugander M, Mosén H, Buhre T, Arheden H. Atrioventricular plane displacement is the major contributor to left ventricular pumping in healthy adults, athletes, and patients with dilated cardiomyopathy Am J Physiol Heart Circ Physiol. 2007 Mar;292(3):H1452-9.
Figures