2111
Four-dimensional whole-heart cine imaging with isotropic resolution in one single breath-hold: initial results1Advanced Clinical Imaging Technology, Siemens Healthcare AG, Lausanne, Switzerland, 2Department of Radiology, University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 3LTS5, École Polytechnique Fédérale de Lausanne (EPFL), Lausanne, Switzerland, 4Center for Biomedical Imaging (CIBM), Lausanne, Switzerland, 5Division of Cardiology and Cardiac MR Center, University Hospital of Lausanne (CHUV), Lausanne, Switzerland
Synopsis
In cardiac MRI, the evaluation of left ventricular ejection fraction (LVEF) is based on well-defined protocols and involves a stack of 2D cine images acquired during multiple breath-holds. This procedure is time-consuming and may result in suboptimal coverage and inter-slice misregistration. Here, a novel acquisition protocol for 3D cine imaging with whole-heart coverage in one single breath-hold with isotropic spatial resolution is described and tested in 10 subjects in comparison to the 2D gold-standard. All 2D datasets and 9/10 3D datasets were considered adequate for LVEF calculation. Bland-Altman analysis of LVEF shows good agreement and no bias between the two measurements.
Introduction
Left ventricular ejection fraction (LVEF) is a very important measure in cardiology and is part of nearly every cardiac imaging evaluation as it shows very high correlation with outcome [1]. In cardiac MRI, the evaluation of LVEF is based on well-defined protocols and involves a stack of double-oblique 2D short-axis cine images that are acquired over multiple breath-holds [2,3]. However, this procedure has several disadvantages. Firstly, the total acquisition time can easily amount to 10min and is determined by slice positioning, the duration of data collection, and by the mandatory pauses in-between serial breath-holds. Secondly, the coverage of the left ventricle (LV) is spatially limited and offers only an approximate assessment of the base of the heart. Lastly, multiple breath-holds are often prone to misalignments between adjacent slices, which may adversely affect the LVEF calculation. To address these limitations, accelerated 3D cine imaging performed in a single breath-hold has been proposed in several flavors, from a multi-slice approach [4-7], to volumetric acquisitions with limited anatomical coverage and anisotropic spatial resolution [8]. Here, a novel acquisition and reconstruction protocol is proposed based on a Free-running framework for 3D cine imaging with whole-heart coverage and isotropic spatial resolution (< 2mm) during one single breath-hold.Materials and Methods
Non-triggered
3D cine acquisitions were performed on a clinical 1.5T scanner (MAGNETOM Aera,
Siemens Healthcare, Erlangen, Germany) in 5 healthy volunteers (3 female, 26±3 years old) and 5 patients (2 female, 44±21 years old) with a modified version of
the prototype sequence described in [9] and using the 3D radial trajectory of
[10]. In volunteers, the protocol was set to a breath-hold duration of 28.5
seconds, in which 8866 radial lines were subdivided into 403 segments of 22
readouts each. In patients, the breath-hold acquisition was performed after
contrast medium injection (0.2mmol/kg Gadobutrol, Gadovist, Bayer Healthcare, Germany) supporting a
reduced acquisition duration of 21 seconds and 6540 acquired radial lines,
subdivided into 327 segments of 20 readouts each. For all 3D acquisitions the
following sequence parameters were used: field-of-view (FOV) (220mm)3,
matrix 1123, isotropic spatial resolution (1.96mm)3,
receiver bandwidth 992 Hz/px, and TE / TR = 1.6/3.2ms. Cine 3D
reconstructions were performed using a similar method to that described in
[11], using the trigger time recorded from the ECG for cardiac binning and with
a temporal resolution of 50ms without view sharing. For gold-standard
comparison, a stack of short axis 2D-cine slices was acquired pre-contrast
during multiple breath-holds with the following sequence parameters: FOV
(300x240)mm, matrix 256x180, in-plane resolution of 1.2x1.2mm, slice thickness
8mm, bandwidth 930Hz/px, and TE/TR = 1.3/3.1ms. Total acquisition and
reconstruction times were recorded. The image quality for function and volume
analysis was visually assessed for both acquisitions. The 3D datasets were then
interpolated and reformatted to match orientation and position of the stack of
2D cine images for quantitative analysis. LVEF was computed for both sets of images using
the Argus VF software (Siemens AG), applying the Simpson rule.
Results
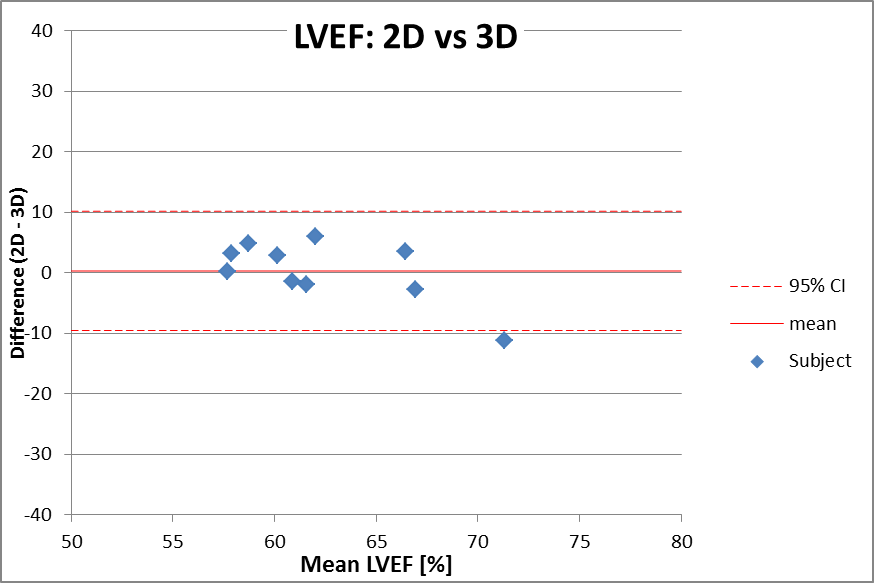
The acquisitions and reconstructions of all 3D breath-hold volumes were successfully performed and the average reconstruction time was 25±5 min. Acquisition time for the 2D cine, including localizers, was 11.4±1.4min on average compared to the 21-28s of the 3D scan. Following visual data inspection, all 2D datasets (n=10) and 9/10 3D data sets were considered adequate for LVEF and LV volume calculation. An example of 3D patient dataset was reconstructed using all k-lines, before binning in cardiac phases, to show image quality achieved with the current amount of undersampling and without compressed sensing (Fig.1). By contrast, an example showing spatio-temporal resolution and image quality obtained after compressed sensing reconstruction is shown in Fig.2 and Fig.3 for a volunteer and a patient, respectively. A comparison between reformatted slices from one subject is shown in Fig.4. The 3D acquisition yielded a similar LVEF of 62.2±6.4% versus 62.5±3.4% measured by the standard technique (p=0.84). The Bland-Altman plot for LVEF is displayed in Fig.5 and shows good correlation with no bias between the two measurements.Discussion and Conclusions
Initial
evaluation of a proposed 3D cine single breath-hold technique shows a good
quantitative agreement for the evaluation of LVEF in comparison with the
clinical gold standard. Further comparisons of both techniques with the stroke
volume measured by 2D flow as described in [12] are warranted when using the
whole 3D volume for LVEF calculation. Reconstruction weights will also undergo
further optimization to find the best compromise between image quality,
precision, and breath-hold duration. In conclusion, it was demonstrated that
accurate LVEF estimation is feasible using free-running 3D cine MRI acquired in
one single breath-hold, but further steps are needed to fully explore the
clinical utility of this techniqueAcknowledgements
No acknowledgement found.References
[1] Curtis JP, et al. The association of left ventricular ejection fraction, mortality, and cause of death in stable outpatients with heart failure. J Am Coll Cardiol 2003;42:736–42.
[2] Kramer C, et al. Standardized cardiovascular magnetic resonance (CMR) protocols 2013 update. J Cardiovasc Magn Reson 2013;15:91.
[3] Kilner PJ, et al. Recommendations for cardiovascular magnetic resonance in adults with congenital heart disease from the respective working groups of the European Society of Cardiology. Eur Heart J 2010;31:794–805.
[4] Wintersperger BJ, et al. Single breath-hold real-time cine MR imaging: improved temporal resolution using generalized autocalibrating partially parallel acquisition (GRAPPA) algorithm. Eur Radiol. 2003; 13:1931.
[5] Kozerke S, et al. Accelerating cardiac cine 3D imaging using k‐t BLAST. Magn Reson Med. 2004; 52: 19-26.
[6] Makowski M, et al. Single breath-hold assessment of cardiac function using an accelerated 3D single breath-hold acquisition technique - comparison of an intravascular and extravascular contrast agent. J Cardiovasc Magn Reson. 2012; 14:53.
[7] Jeong D, et al. Single breath hold 3D cardiac cine MRI using kat-ARC: preliminary results at 1.5T. Int J Cardiovasc Imaging. 2015; 31:851.
[8] Wetzl J, et al. Single-breath-hold 3-D CINE imaging of the left ventricle using Cartesian sampling. Magn Reson Mater Phy Biol Med. 2018; 31:19-31.
[9] Coppo S, et al. Free-running 4D whole‐heart self‐navigated golden angle MRI: Initial results. Magn Reson Med. 2015; 74:1306-1316.
[10] Piccini D, et al. Spiral phyllotaxis: The natural way to construct a 3D radial trajectory in MRI. Magn Reson Med. 2011; 66:1049-1056.
[11] Feng L, et al. 5D whole‐heart sparse MRI. Magn Reson Med. 2018; 79: 826-838.
[12] Vincenti G, et al. Compressed Sensing Single–Breath-Hold CMR for Fast Quantification of LV Function, Volumes, and Mass. J Am Coll Cardiol-Imaging. 2014; 7:882-892.
Figures