2109
Elimination or Minimization in Depth of Sedation in Pediatric Cardiac Patients Considered High-Risk for Anesthesia: Using CArdioREspiratory Synchronized (CARESync) Balanced Steady-State Free Precession Cine Imaging1Texas Children's Hospital, Houston, TX, United States
Synopsis
General anesthesia (GA), while not always required, is frequently necessary in infants and children undergoing cardiac magnetic resonance imaging (CMR) based on risk-benefit of breath-hold under GA v/s diagnostic value of the images. Primarily, requirement of breath-hold for cine imaging to evaluate ventricular volumes and function, a key prognostic measure in spectrum of congenital heart diseases, governs the administration of anesthesia. Our experience demonstrates that completely free-breathing-CMR studies including CArdio-REspiratory Synchronized cine imaging allow elimination of anesthesia or minimization in depth of sedation while providing diagnostic morphologic, functional, and pathophysiologic evaluation in young children, and adolescents considered high-risk for anesthesia.
PURPOSE
To review the role of completely free breathing cardiac MRI studies, including CArdio-REspiratory Synchronized (CARESync) cine imaging, in eliminating anesthesia completely or lower the depth of sedation in pediatric cardiac patients considered high-risk for anesthesia.INTRODUCTION
Cardiovascular magnetic resonance (CMR) imaging is the current clinical gold standard for measurements of ventricular function and blood flow, both, crucial components in assessment of CHD [1]. There are several forms of CHD, particularly those initially palliated, that are heavily impacted by quantification of ventricular volumetric and functional indices [2,3]. However, routine clinical cine balanced steady-state free precession (bSSFP) CMR imaging requires suspension of respiration to obtain diagnostic image quality with adequate spatio-temporal resolution. Thus, general anesthesia (GA), while not always required, is frequently necessary in infants and children undergoing CMR based on risk-benefit of breath-hold under GA v/s diagnostic value of the acquired images. Diagnostic image quality and accuracy of ventricular volumetric and functional indices of a free breathing respiratory synchronized bSSFP sequence, without contrast administration and with real-time reconstruction, has been reported in pediatric and adult populations [4, 5]. CARESync further enables acquisition throughout expiration [6]. This report reviews our experience of completely free-breathing-CMR studies including CARESync Synchronized cine imaging, in pediatric population considered as high-risk for anesthesia.METHODS
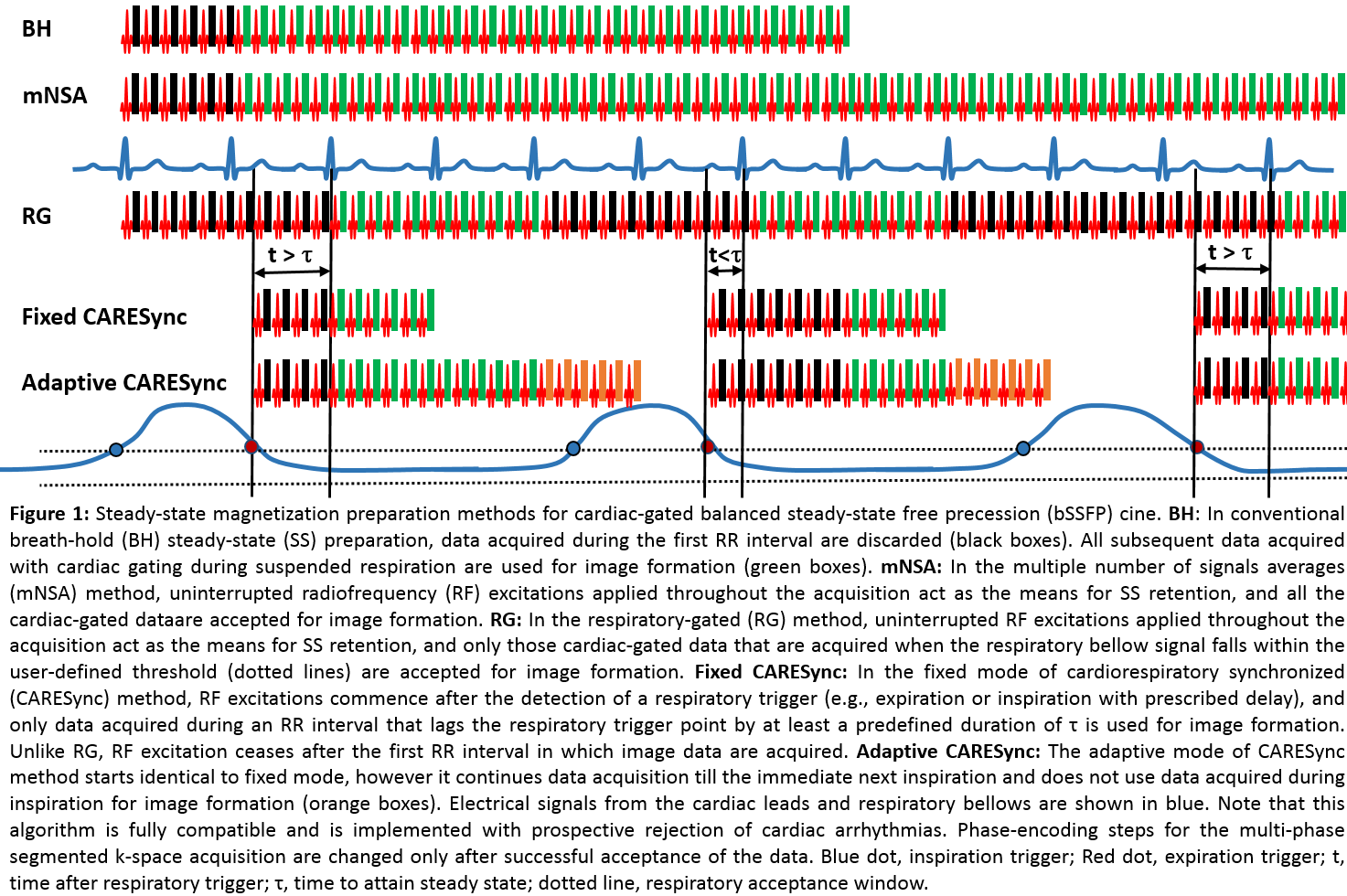
We retrospectively reviewed the anesthesia and MRI records for all patients who had undergone CMR between June 2017 and September 2018 on three 1.5T clinical MR scanners at our institute. Patients requiring sedation received either intravenous (IV) sedative, chiefly Propofol, or general anesthesia (GA), chiefly Sevoflurane. All imaging with CARESync was IRB approved with waiver for patient consent and was performed on a 1.5T clinical MR scanner (Ingenia, Philips Healthcare). CARESync sequence described in Fig1 allows two free breathing modes: fixed – single R-R per respiration, and adaptive – multiple R-R per respiration with prospective rejection for inspiration during acquisition. The imaging parameters were: TR/TE/FA=2.5-2.7ms/1.25-1.35ms/60°; acquired voxel size: 1.65-2x1.65-2x5-8 mm3; SENSE=1.3-2; temporal resolution 30-45ms.RESULTS
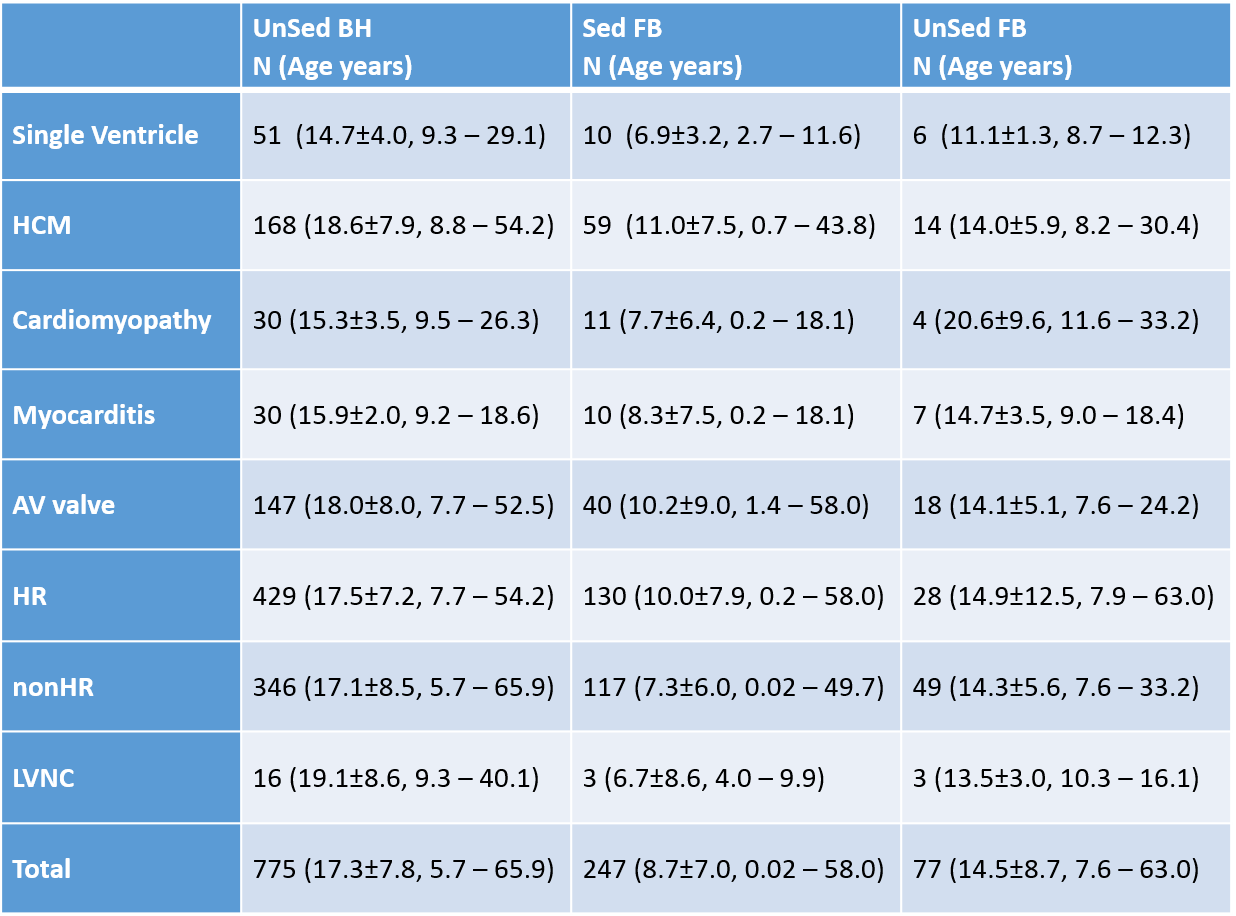
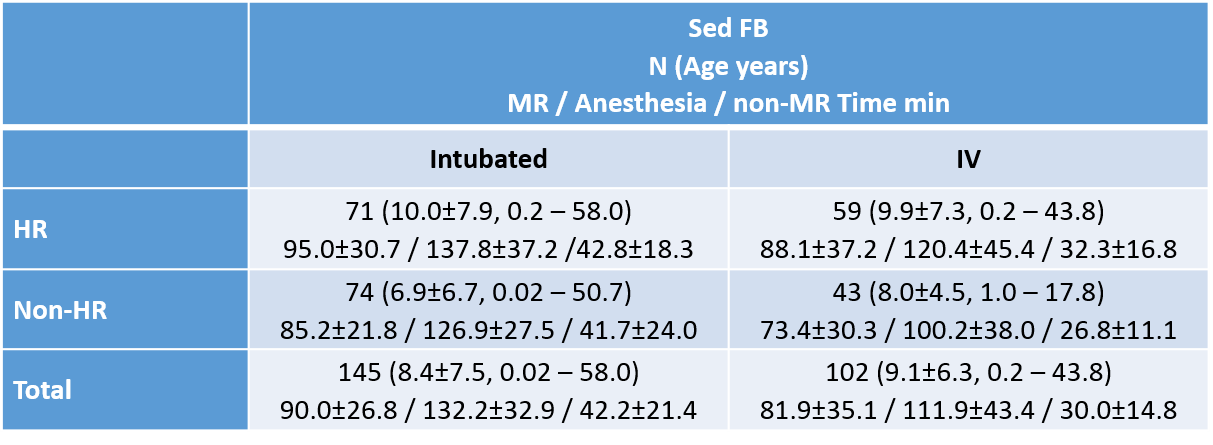
A total of 324 out of 1100 patients underwent FB-CMR as they were unable to hold their breath. All the CMR studies were completed without complications due to hemodynamic or respiratory instability and provided diagnostic image quality. Patients considered high-risk (HR) for anesthesia (BH/FB) included: single ventricles (51/16), hypertrophic cardiomyopathy (168/73), cardiomyopathy with moderate-to-severely depressed function (30/15), myocarditis (30/17), and atrioventricular valve diseases including, moderate-to-sever aortic insufficiency, aortic regurgitation, or mitral stenosis (147/58). A total of 77(14.5±8.7, 7.6-63.0 yrs) FB-CMR studies performed without any anesthesia included 28(14.9±12.5, 7.9-63.0 yrs) HR patients. Out of 247(8.7±7.0, 0.02-58.0 yrs) sedated FB-CMR studies 130(10.0±7.7, 0.2-58.0 yrs) were HR, comprised of 59(9.9±7.3, 0.2-43.8 yrs) with IV and 71(10.0±7.9, 0.2-58.0 yrs) with GA. Twenty two (17.5±3.0, 4.0 – 40.1yrs) patients were indicated for left ventricular non-compaction (LVNC). Average CMR imaging times (HR-IV 95.0±30.7 min, HR-GA 88.1±37.2) and additional anesthesia times (HR-IV 32.3±16.8 min, HR-GA 42.8±18.3) for HR-IV and HR-GA patients were comparable.CONCLUSION
Our experience demonstrates that complete FB-CMR studies including CARESync cine imaging allow elimination of anesthesia or minimization in depth of sedation while providing diagnostic morphologic, functional and pathophysiologic evaluation in young children, and adolescents considered high-risk for anesthesia. CARESync has been previously reported to improve image quality significantly over MSA and provide comparable ventricular volumes [4]. Furthermore, superior delineation of trabeculation and myocardium from blood pool allows accurate measurements of non-compacted and compacted myocardium critical for hypertrophic cardiomyopathy and left ventricular non-compaction. Retrospectively gated acquisition with adequate spatio-temporal resolution provides overall better wall motion assessment. Elimination of breath-holds in CMR minimizes the risk of respiratory depression and airway obstruction, without affecting the cardiac output in patients with limited cardiovascular reserve. It may be worthwhile to explore increased utilization of FB-CMR with highly accelerated techniques to further reduce need for anesthesia.Acknowledgements
No acknowledgement found.References
[1] Valsangiacomo Buechel ER, Grosse-Wortmann L, Fratz S, Eichhorn J, Sarikouch S, Greil GF, et al. Indications for cardiovascular magnetic resonance in children with congenital and acquired heart disease: an expert consensus paper of the Imaging Working Group of the AEPC and the Cardiovascular Magnetic Resonance Section of the EACVI. Eur Heart J - Cardiovasc Imaging. 2015;16:281–97.
[2] Bokma JP, Winter MM, Oosterhof T, Vliegen HW, van Dijk AP, Hazekamp MG, et al. Preoperative thresholds for mid-to-late haemodynamic and clinical outcomes after pulmonary valve replacement in tetralogy of Fallot. Eur Heart J. 2016;37:829–35.
[3] Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Guyton RA, et al. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:2440–92.
[4] Krishnamurthy R, Pednekar A, Atweh LA, Vogelius E, Chu ZD, Zhang W, et al. Clinical validation of free breathing respiratory triggered retrospectively cardiac gated cine balanced steady-state free precession cardiovascular magnetic resonance in sedated children. J Cardiovasc Magn Reson. 2015;17. doi:10.1186/s12968-014-0101-1.
[5] Pednekar AS, Wang H, Flamm S, Cheong BY, Muthupillai R. Two-center clinical validation and quantitative assessment of respiratory triggered retrospectively cardiac gated balanced-SSFP cine cardiovascular magnetic resonance imaging in adults. J Cardiovasc Magn Reson. 2018;20:44.
[6] Pednekar A. Clinical Validation of Free Breathing CArdioREspiratory Synchronized (CARESynch) Balanced Steady-State Free Precession (bSSFP) Cine Imaging. In: 20th Annual SCMR Scientific Sessions Abstract Supplement. Washington, DC; 2017.
Figures