2108
A fast and semi-automated approach for assessing left ventricular longitudinal strain with cine cardiovascular magnetic resonance imaging in heart failure with preserved and mid-range ejection fraction1National Heart Centre Singapore, Singapore, Singapore, 2Duke-NUS Medical School, Singapore, Singapore
Synopsis
This study aimed to study the left ventricular (LV) longitudinal deformation by a semi-automated and rapid assessable strain parameter (i.e. global longitudinal strain, GLS) with standard cardiovascular magnetic resonance images. Study population consisted of 50 normal controls, 60 patients with heart failure (10 HFpEF, 10 HFmrEF and 40 HFrEF) and 10 patients with hypertrophic cardiomyopathy. Average processing time of the fast strain measurement method was 78 ± 8 seconds per case with intra- and inter-observer variations ranging from 3.3% to 5.8%. Results demonstrated that the fast and reproducible GLS is a powerful independent predictor in patients with HFpEF and HFmrEF.
Background and Purpose
Assessment of left ventricular (LV) systolic longitudinal function has gained increasing diagnostic and prognostic importance as an addition to LV ejection fraction (EF) in patients with heart failure (HF) or hypertrophic cardiomyopathy (HCM).1 Strain imaging derived from speckle tracking echocardiography (STE) or feature tracking cardiovascular magnetic resonance (FT-CMR) enables the direct measurements of myocardial function in the longitudinal direction, however, these parameters often suffer from poor reproducibility and lack of the internal consistency. Therefore, there is unmet need for an automated method that can assess the LV global longitudinal strain (GLS) rapidly and is reproducible.
Methods
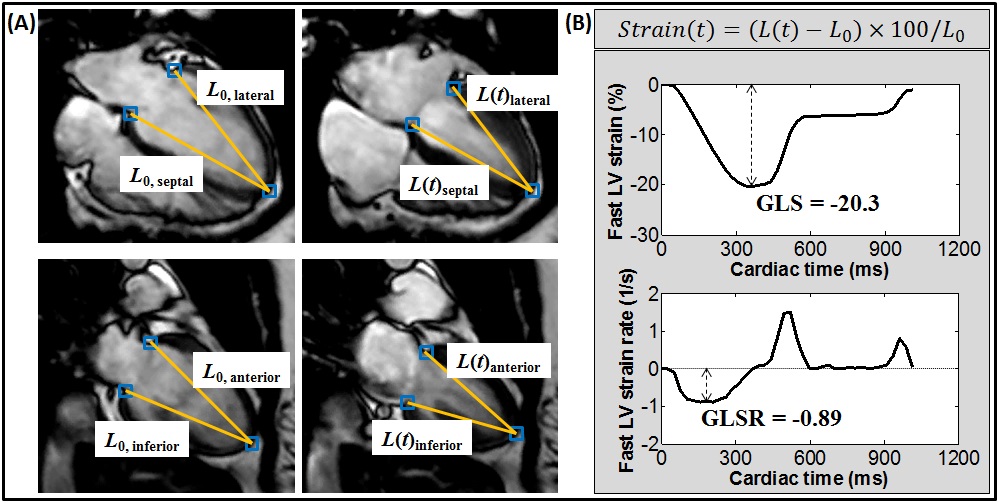
This study enrolled 50 normal controls, and 70 patients (40 HF with reduced EF (HFrEF, LVEF < 40%); 10 HF with mid-range EF (HFmrEF, LVEF 40 – 49%); 10 HF with preserved EF (HFpEF, LVEF ≥ 50%); and 10 HCM). CMR scan was performed on a 3T system (Ingenia, Philips Healthcare) using balanced turbo field echo sequence. End-expiratory breath hold cine images were acquired in multi-planar long-axis views including the two- and four-chamber views. Central off-line assessment of LV volumes was performed using Simpson’s method; and longitudinal LV strain parameters measured using an in-house semi-automatic post-processing algorithm that tracked, on standard two- and four-chamber cine views, the distance ($$$L$$$) between the left atrioventricular junction and apical epicardium (Fig. 1A). The atrioventricular junctions were selected as the mitral valve insertion points at the septal and lateral borders of the annulus on the four-chamber view, and the anterior and inferior annular insertion points on the two-chamber view.2-7 The strain of each wall at any time point ($$$t$$$) in the cardiac cycle from LV end-diastole ($$$t=0$$$) was calculated based on the strain formula: $$$\frac{\left(L(t)-L_{0}\right)\times100}{L_{0}}$$$. The peak systolic GLS was obtained at $$$t$$$ equal to LV end-systole, and the corresponding peak systolic strain rate (GLSR) was derived by taking the first-order derivative of the strain (Fig. 1B). All resulting values from the 4 walls in two- and four-chamber views were then averaged to obtain the global GLS and GLSR of the whole LV. In addition, peak mitral annular velocity during early systole (Sm) and systolic excursion (MAPSE) were calculated based on the tracking of atrioventricular junction.2-5 Student’s t test or Mann-Whitney U test was used for inter-group comparison; p < 0.05 denotes statistical significance. The diagnostic performance of fast LV strain measurements for detecting HFpEF and HFmrEF was assessed using the receiver operating characteristics (ROC) analysis.Results
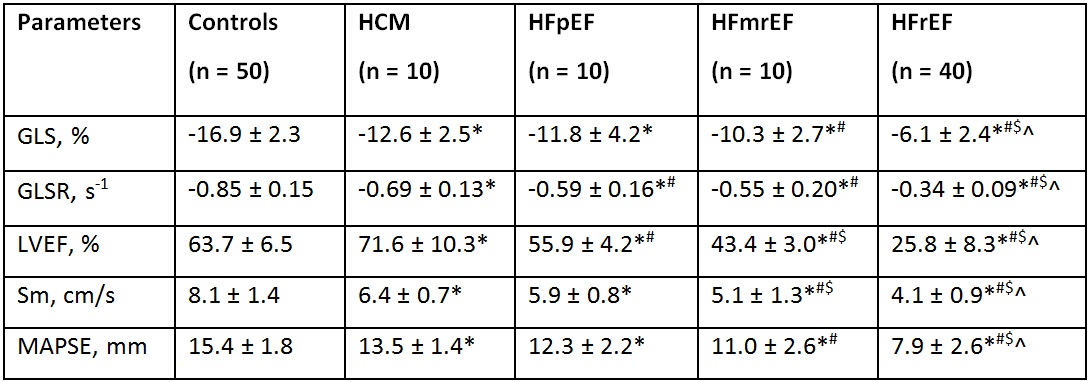
The fast GLS assessment was successfully performed in all cases and the average processing time was 78 ± 8 seconds per case. Intra- and inter-observer variations were ranging from 3.3% to 5.8% (all intra-class correlation coefficient (ICC) > 0.9). Compared with controls, a decreasing trend in GLS and GLSR was observed in patients with HCM, HFpEF, HFmrEF and HFrEF (GLS: normal, -16.9 ± 2.3%; HCM, -12.6 ± 2.5%; HFpEF, -11.8 ± 4.2%; HFmrEF, -10.3 ± 2.7%; HFrEF, -6.1 ± 2.4%; GLSR: normal, -0.85 ± 0.15s-1; HCM, -0.69 ± 0.13s-1; HFpEF, -0.59 ± 0.16s-1; HFmrEF, -0.55 ± 0.20s-1; HFrEF, -0.34 ± 0.09s-1; p < 0.001, Table 1). On multivariate analysis, fast LV GLS was found to be the independent predictor of HFpEF and HFmrEF. The area under the ROC curve (AUC) in detecting HFpEF and HFmrEF compared with normal controls (GLS < 14.0%) was 0.927 (sensitivity = 90%, specificity = 88%, p < 0.001).
Conclusion
This study demonstrated a fast, semi-automated, and robust GLS measurement method for quantifying LV longitudinal function from routine cine CMR images without the need for additional acquisition protocol or special software tool. The fast GLS measurements had superior diagnostic performance compared to conventional LV ejection fraction. In a population with a high suspicion of HFpEF, GLS may significantly contribute to early diagnosis and hence be useful in the triage and management of HFpEF and HFmrEF patients.Acknowledgements
This study received funding support from the National Medical Research Council of Singapore (NMRC/EDG/1037/2011; NMRC/TA/0031/2015; NMRC/OFIRG/0018/2016; NMRC/BnB/0017/2015), Hong Leong Foundation and Edwards Lifesciences.References
- Claus P, Omar AMS, Pedrizzetti G, Sengupta PP, Nagel E. Tissue tracking technology for assessing cardiac mechanics: principles, normal values, and clinical applications. JACC Cardiovasc Imaging. 2015;8:1444-1460.
- Leng S, Zhao XD, Huang FQ, et al. Automated quantitative assessment of cardiovascular magnetic resonance-derived atrioventricular junction velocities. Am J Physiol Heart Circ Physiol. 2015;309:H1923-H1935.
- Leng S, Jiang M, Zhao XD, et al. Three-dimensional tricuspid annular motion analysis from cardiac magnetic resonance feature-tracking. Ann Biomed Eng. 2016;44:3522-3538.
- Leng S, Zhang S, Jiang M, et al. Imaging 4D morphology and dynamics of mitral annulus in humans using cardiac cine MR feature tracking. Sci Rep. 2018;8:81.
- Leng S, Zhao XD, Koh AS, et al. Age-related changes in four-dimensional CMR-derived atrioventricular junction velocities and displacements: implications for the identification of altered annular dynamics for ventricular function assessment. Int J Cardiol Heart Vasc. 2018, in press.
- Leng S, Tan RS, Zhao XD, Allen JC, Koh AS, Zhong L. Validation of a rapid semi-automated method to assess left atrial longitudinal phasic strains on cine cardiovascular magnetic resonance imaging. J Cardiovasc Magn Reson. 2018;20:71.
- Koh AS, Gao F, Leng S, et al. Dissecting clinical and metabolomics associations of left atrial phasic function by cardiac magnetic resonance feature tracking. Sci Rep. 2018;8:8138.
Figures