2106
Fully Self-Gated Cardiac and Respiratory Motion-Resolved 5D MRI for Rapid Assessment of Left Ventricular Function1Department of Diagnostic and Interventional Radiology, Lausanne University Hospital (CHUV and UNIL), Lausanne, Switzerland, 2Center for Biomedical Imaging (CIBM), Lausanne, Switzerland, 3Division of Cardiology and Cardiac MR Center, Lausanne University Hospital (CHUV and UNIL), Lausanne, Switzerland, 4Advanced Clinical Imaging Technology, Siemens Healthcare AG, Lausanne, Switzerland
Synopsis
Cardiac magnetic resonance is the gold standard for left ventricular (LV) function assessment; however, current clinical protocols follow a rather complex workflow to plan and to acquire standard short-axis cine MR images. To simplify the workflow and remove these hurdles, we implemented and validated a time efficient free-running, free-breathing, fully self-gated cardiac and respiratory motion-resolved 5D MRI framework with isotropic spatial resolution. Assessment of LV function using the proposed framework and conventional 2D cines demonstrated good agreement between both techniques. When compared to the conventional approach, the proposed framework improves time efficiency and facilitates workflow.
Introduction
Left ventricular function is a strong predictor of outcome in patients with heart failure1 and an important measurement to guide and monitor therapy. Cardiac magnetic resonance (CMR) has improved significantly over the last decade2-4 and is now generally accepted as the gold standard for LV function assessment. Recent advances have enabled assessment of LV function using a single-breath-hold 3D Cartesian acquisition with limited coverage and spatial resolution.4 While these 3D Cartesian data can be reformatted in any orientation, their non-isotropic, low spatial resolution may be suboptimal for accurate assessment of LV function. Moreover, prolonged breath-hold acquisitions are often challenging for patients and may even result in Valsalva maneuvers which results in incorrect function assessment. Long breath-holds may also prevent functional assessment in non-compliant subjects. In addition, operator involvement remains considerable as several cardiac localizers are still necessary to find the short-axis view. To remove these constraints and to simplify workflow, we propose a fully self-gated cardiac and respiratory motion-resolved 5D MRI framework5 with improved time efficiency and isotropic spatial resolution for LV function assessment.Methods
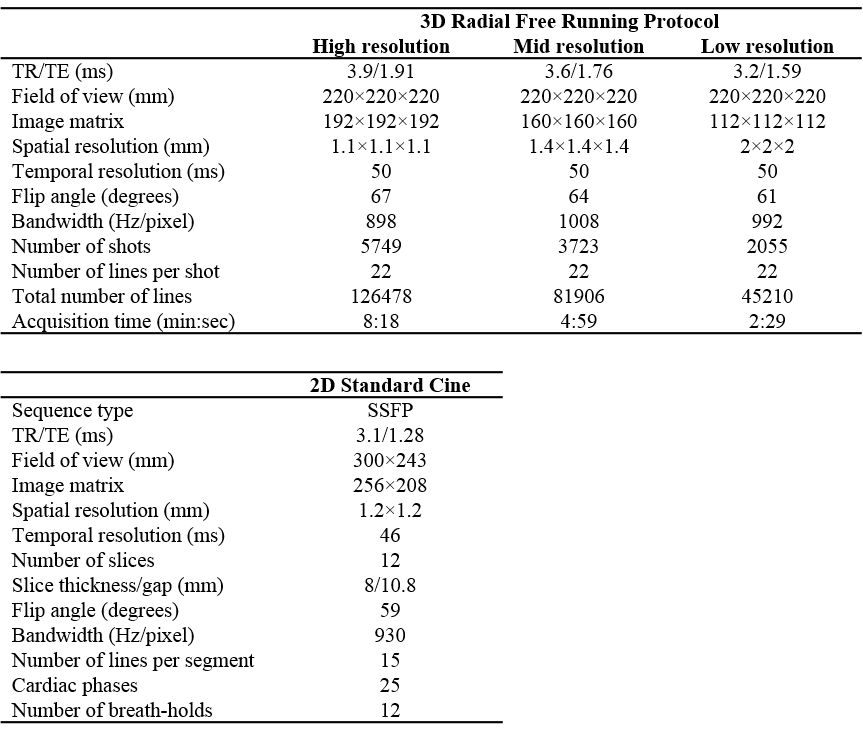
The framework was validated in four volunteers and three patients. All examinations were performed on a 1.5T MRI scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). The accuracy of the proposed framework to measure LV ejection fraction (LVEF) were compared to a standard multislice high-resolution SSFP cine CMR approach. The imaging protocol consisted of several localizers followed by a stack of conventional 2D short-axis SSFP cine images covering the entire LV (Table in Fig.1). For the proposed CS-based framework, data were acquired with a prototype free-running non-ECG-triggered 3D golden-angle radial sequence (Table in Fig.1). To improve the duty cycle when compared to our earlier approach,5 fat saturation and ramp-up pulses were removed. Three datasets with different spatial resolutions were acquired for each volunteer. Due to time constraints, only one dataset could be acquired per patient and, therefore, we tested a different spatial resolution in each patient.
Cardiac and respiratory self-gating signals6 were obtained to sort the data into 4 respiratory states and 14-23 cardiac phases (50ms temporal resolution). The resultant 5D (x-y-z-cardiac-respiratory dimensions) datasets were reconstructed using k-t sparse SENSE with regularization along both cardiac and respiratory dimensions.5 Regularization weights were carefully optimized to prevent compression artifacts that could potentially affect LVEF measurements.
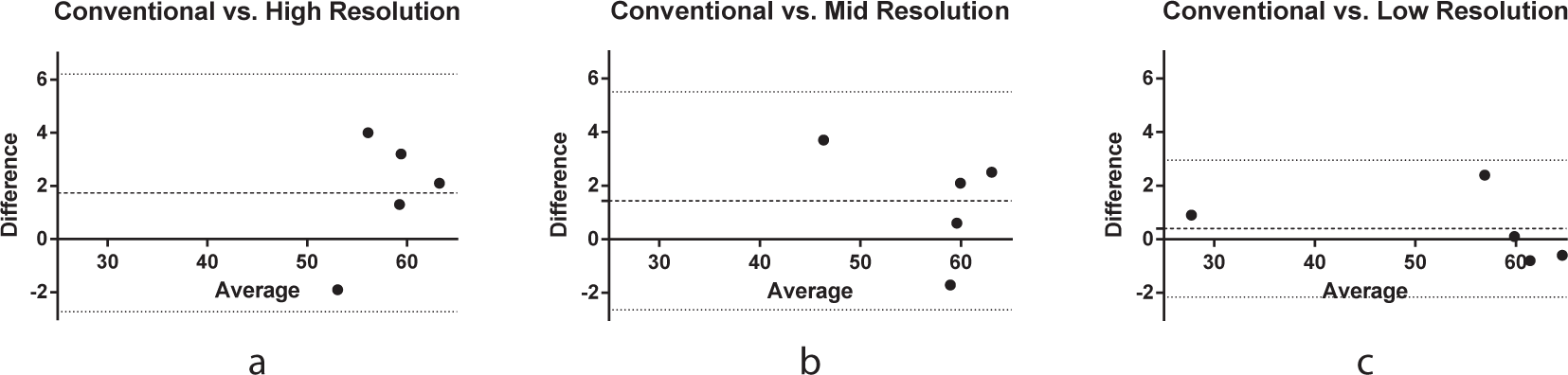
Slice orientations and positions of the conventional stacks of short-axis cine images were used to guide multiplanar reformatting in the 5D motion-resolved CS datasets. The conventional and multiplanar reformatted stacks of short-axis cine MR images were then analyzed with Argus VF software (Siemens AG) by a cardiologist to measure LVEF.7 Bland-Altman plots, and one-way ANOVA were used to evaluate the correlation and agreement between the different measurements. Total acquisition time was recorded. The image quality for conventional and multiplanar reformatted stacks of short-axis cine MR images was visually assessed.
Results
Fully self-gated cardiac and respiratory motion-resolved 5D images were successfully reconstructed with the proposed automated framework for all volunteers, patients, and investigated spatial resolutions. The approach effectively suppressed motion artifacts for both volunteers (Fig.2) and patients (Fig.3). Multiplanar cine reformats extracted in a short axis view from the 5D CS data showed a strong agreement with the conventional stack of short-axis images (Fig. 3) in both anatomy and function. Quantitative LV function assessment obtained from the conventional and the 5D CS cine images yielded good agreement for ejection fraction measures for all investigated spatial resolutions with no significant bias (Fig.5; p=0.88 for the mean difference in LVEF). Finally, acquisition time for the conventional 2D stack (including localizers + rest between breath-holds) was 14.4±4.6min on average compared to 8min18s, 4min59s, and 2min29s for the three different the 5D protocols.Discussion and Conclusions
An automated CS framework for fully
self-gated free-running 5D MRI of the heart without the need for gating,
navigation, ECG triggering, or contrast media was successfully implemented and
tested for LV functional assessment. When compared to conventional clinical
sequences, the proposed 5D CS method improves time efficiency and facilitates
workflow by obviating the need for multiple localizers, multiple breath-holds,
and ECG lead placement. The measured LVEFs were in good agreement with the
measurements from conventional 2D short-axis cine images. The results
demonstrated the feasibility of applying the CS strategy to evaluate LV
function in as little as 2min29s. In this work, we reformatted 3D isotropic
images to match the current standard 2D technique. However, a true 3D cardiac
function measurement should allow for more accurate assessment of cardiac function
as it may track atrioventricular valve motion more accurately.Acknowledgements
No acknowledgement found.References
1. Curtis, J. P. et al. The association of left ventricular ejection fraction, mortality, and cause of death in stable outpatients with heart failure. J Am Coll Cardiol 42, 736-742 (2003).
2. Liu, J. et al. Highly-accelerated self-gated free-breathing 3D cardiac cine MRI: validation in assessment of left ventricular function. MAGMA 30, 337-346, doi:10.1007/s10334-017-0607-2 (2017).
3. Kido, T. et al. Compressed sensing real-time cine cardiovascular magnetic resonance: accurate assessment of left ventricular function in a single-breath-hold. J Cardiovasc Magn Reson 18, 50, doi:10.1186/s12968-016-0271-0 (2016).
4. Wetzl, J. et al. Single-breath-hold 3-D CINE imaging of the left ventricle using Cartesian sampling. MAGMA 31, 19-31, doi:10.1007/s10334-017-0624-1 (2018).
5. Feng, L. et al. 5D whole-heart sparse MRI. Magn Reson Med, doi:10.1002/mrm.26745 (2017).
6. di Sopra, L. et al. Motion-Resolved 5D Imaging of the Heart: Time to Get Rid of the ECG?. in Proc Intl Soc Mag Reson Med 24. 3148 (2017).
7. Vincenti, G. et al. Compressed sensing single-breath-hold CMR for fast quantification of LV function, volumes, and mass. JACC Cardiovasc Imaging 7, 882-892, doi:10.1016/j.jcmg.2014.04.016 (2014).
Figures