2103
Cardiac Strains from DENSE MRI: Evaluation of SNR Requirements and Strain Error using a Computational Phantom1Radiological Sciences Laboratory, Stanford University, Stanford, CA, United States, 2Radiological Sciences, University of California - Los Angeles, Los Angeles, CA, United States
Synopsis
Displacement Encoding with Stimulated Echoes (DENSE) MRI encodes high-resolution cardiac tissue displacements into the phase of the complex MR signal. However, due to the inherent difficulty of obtaining ground truth strain measurements in the beating heart, it remains unclear how image SNR impacts the bias and range of error for computed cardiac strains. In this work, we present a computational deforming heart-like phantom to evaluate cardiac strains computed using a widely available, open-source DENSE Image Analysis Tool. We show that a strain error range within 0.05 and near-zero median error bias can be achieved with SNR>20.
Introduction
Displacement Encoding with Stimulated Echoes (DENSE) MRI encodes tissue displacements into the phase of the complex MR signal. Due to its high spatial and temporal resolution, DENSE MRI is effective for measuring regional cardiac strains in the clinic1,2 and in preclinical modeling studies evaluating myocardial stiffness3 and kinematics4.
Different encoding strategies have been proposed to minimize phase variance and maximize signal-to-noise ratio (SNR) in the acquired DENSE images. Although these encoding strategies have been validated using gel phantoms5, it remains unclear how image SNR specifically impacts measured cardiac strains along the circumferential (Ecc), radial (Err), longitudinal (Ell) and cardiomyocyte aggregate (i.e. “fiber”) (Eff) directions. This is due to the inherent difficulty of obtaining ground truth strain measurements in the beating heart.
The objectives of this work were: 1) to quantify the accuracy and precision of cardiac strains computed using the most widely available, open-source DENSE Image Analysis Tool6; and 2) to quantify how image SNR propagates through the encoding and processing pipeline to impact the bias and range of computed Ecc, Err, Ell and Eff.
Methods
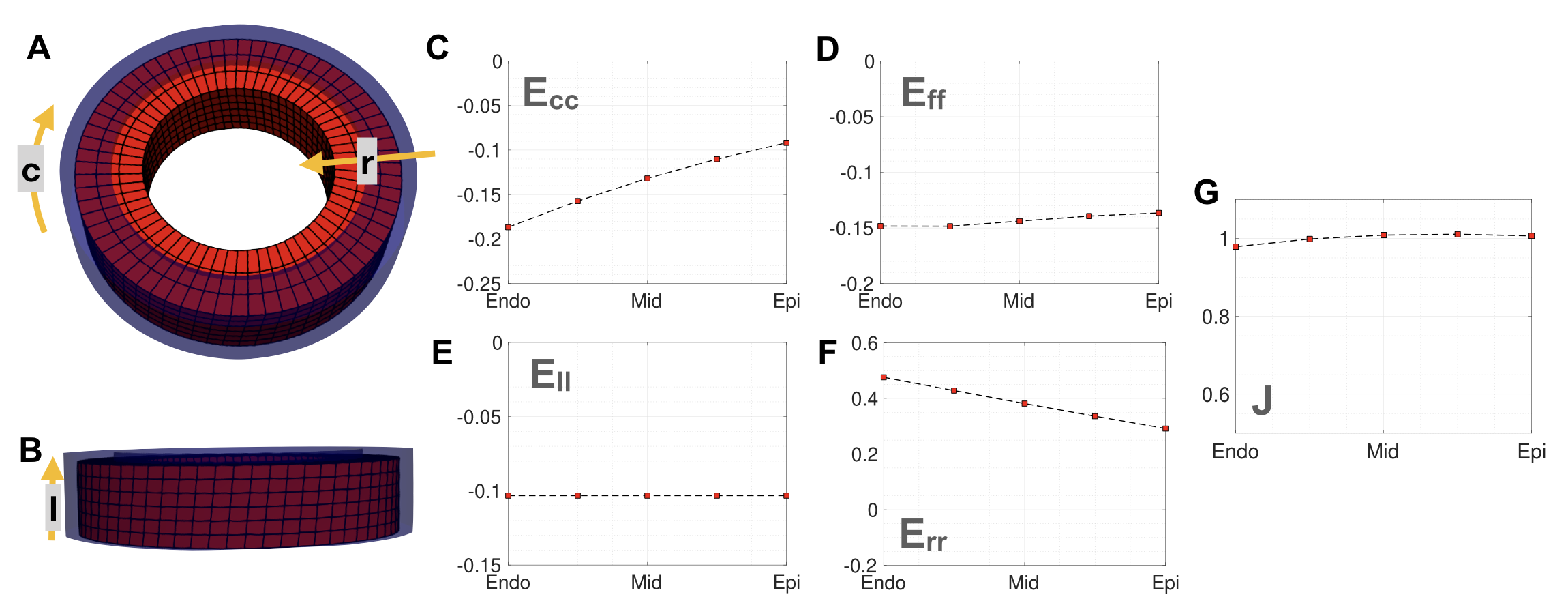
We use an axial-symmetric deforming heart-like computational phantom with time-resolved deformation defined by three analytical functions for radial, circumferential, and longitudinal motion. The target ground-truth peak systolic strains were calibrated based on strain reports from in vivo DENSE studies8 (Fig. 1).
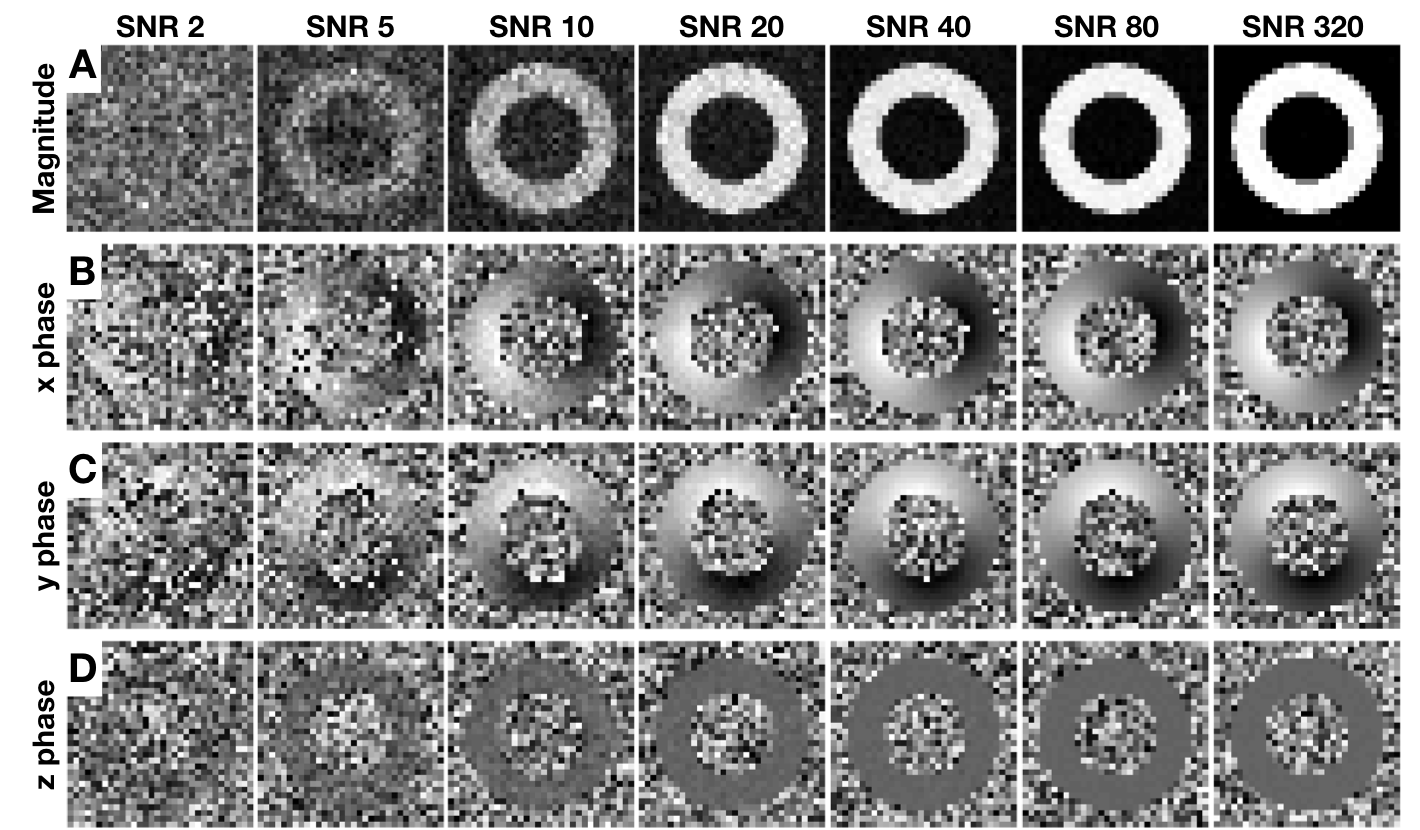
The phantom deformation field was subdivided into a grid of 2.5x2.5x8mm voxels at two slice locations, spaced 8mm from each other. To account for intravoxel dephasing and partial volume effects, Eulerian tissue displacements were sampled at 12 points within each voxel, and averaged to generate a bulk displacement vector per voxel. The corresponding phase was computed by scaling the bulk displacement components according to an encoding strength of 0.08 cycles/mm. The signal magnitude was computed as the average magnitude across all intravoxel sampling points, assuming a signal of 0 for air and 1 for myocardium (Fig. 2A).
DENSE imaging typically employs a balanced 4-point encoding scheme. To properly account for noise, the phantom displacements were transformed into the corresponding balanced 4-point phase maps according to the encoding matrix outlined in Zhong et al.5 Complex valued noise was added to the four phase maps for a range of ten different SNRs (SNR = 2 - 320). Finally, the resulting noise-injected complex images were encoded back into phase along x, y, and z (Fig. 2B-D). Each SNR simulation was repeated five times for strain analysis.
Lagrangian phantom displacements in x, y and z were extracted from the signal phase using the DENSE Image Analysis Tool6. Using a mesh-free interpolation scheme7, myocardial Ecc, Err, Ell, and Eff between the two simulated slice locations were computed at 200 points and across the range of DENSE SNRs. Pointwise strain difference, defined as ground truth strain minus computed DENSE strain, was measured at all 200 sampled points for each SNR repetition and quantified through the heart wall. We set a target of near-zero strain bias and a strain error range within 0.05.
Results
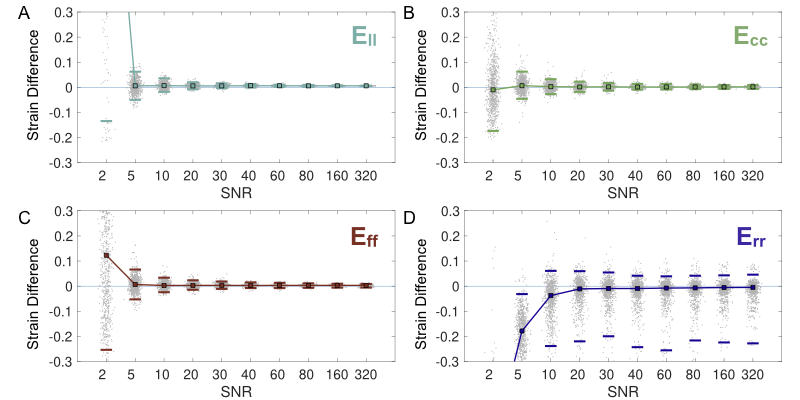
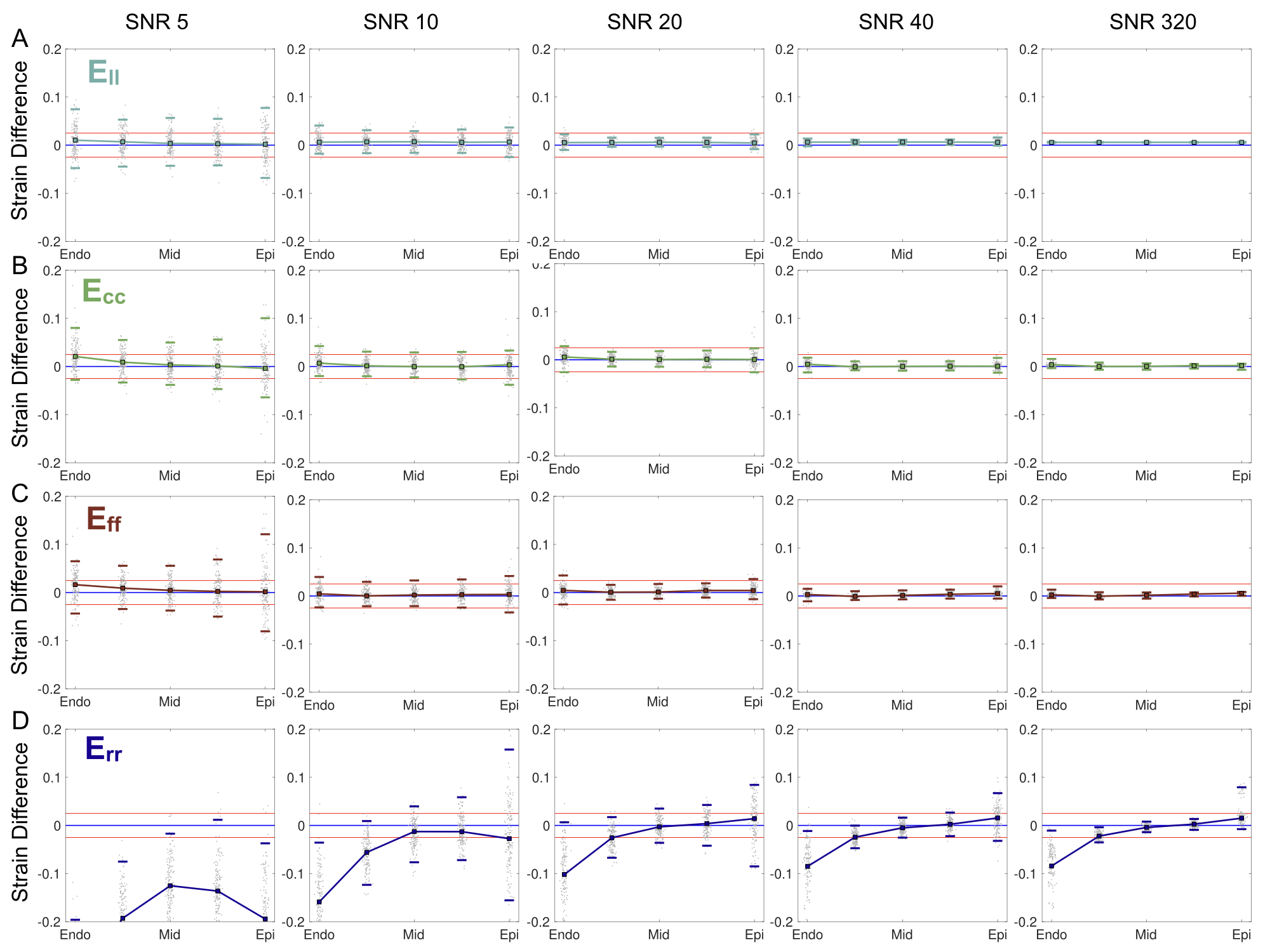
Eff, Ecc, Ell, and mid-wall Err exhibit near-zero median strain bias across SNRs (Fig. 4). Epicardial and endocardial Err showed a strain bias of -0.08 and +0.01 at the endocardium and epicardium, respectively.
The 95%-confidence interval (95%-CI) of strain differences for Eff, Ecc, Ell, and mid-wall Err tightens within the target range of 0.05 for SNR>20 (Fig 4D). 95%-CI of epi- and endocardial Err error does not converge within 0.05.
Discussion
At SNR = 320, the median and range of strain error is near-zero for Eff, Ecc, and Ell, indicating the DENSE Analysis Tool accurately and precisely characterizes these cardiac strains (Fig. 3). Err exhibited pronounced computed strain bias and a broad 95%-CI even at SNR = 320 (Fig. 4). It remains to be investigated if Err is therefore more susceptible to voxel size and/or the numerical method used to differentiate the DENSE displacement field.
This study demonstrates that the precision of computed strains, and not the bias, is primarily impacted by image SNR. The measured impact of SNR on strain precision can help guide analysis of longitudinal clinical studies of DENSE MRI strains.
Conclusion
We find that Eff, Ecc, Ell and mid-wall Err are computed with near-zero median bias and within a strain error range of 0.05 for SNR>20. The flexibility of our validation pipeline allows for future assessment of the impact that other imaging parameters (e.g., resolution, encoding strength, number of encoding directions) have on measured cardiac strains. These simulations can provide a priori estimates of required protocol parameters to achieve a target strain sensitivity in clinical studies.Acknowledgements
Funding support from NIH K25 HL135408, NIH R01 HL131975 and NIH R01 HL131823.References
1 - Aletras AH, Tilak GS, Hsu LY, Arai AE. Heterogeneity of Intramural Function in Hypertrophic CardiomyopathyClinical Perspective: Mechanistic Insights From MRI Late Gadolinium Enhancement and High-Resolution Displacement Encoding With Stimulated Echoes Strain Maps. Circulation: Cardiovascular Imaging. 2011 Jul 1;4(4):425-34.
2 - Bilchick KC, Kuruvilla S, Hamirani YS, Ramachandran R, Clarke SA, Parker KM, Stukenborg GJ, Mason P, Ferguson JD, Moorman JR, Malhotra R. Impact of mechanical activation, scar, and electrical timing on cardiac resynchronization therapy response and clinical outcomes. Journal of the American College of Cardiology. 2014 Apr 29;63(16):1657-66.
3 - Perotti LE, Ponnaluri AV, Krishnamoorthi S, Balzani D, Ennis DB, Klug WS. Method for the unique identification of hyperelastic material properties using full‐field measures. Application to the passive myocardium material response. International journal for numerical methods in biomedical engineering. 2017 Nov;33(11):e2866.
4 - Perotti LE, Magrath P, Verzhbinsky IA, Aliotta E, Moulin K, Ennis DB. Microstructurally Anchored Cardiac Kinematics by Combining In Vivo DENSE MRI and cDTI. In International Conference on Functional Imaging and Modeling of the Heart 2017 Jun 11 (pp. 381-391). Springer, Cham.
5 - Zhong X, Helm PA, Epstein FH. Balanced multipoint displacement encoding for DENSE MRI. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2009 Apr;61(4):981-8.
6 - Spottiswoode BS, Zhong X, Hess AT, Kramer CM, Meintjes EM, Mayosi BM, Epstein FH. Tracking myocardial motion from cine DENSE images using spatiotemporal phase unwrapping and temporal fitting. IEEE transactions on medical imaging. 2007 Jan;26(1):15-30. Code available at: https://github.com/denseanalysis/denseanalysis
7 - Arroyo M, Ortiz M. Local maximum‐entropy approximation schemes: a seamless bridge between finite elements and meshfree methods. International journal for numerical methods in engineering. 2006 Mar 26;65(13):2167-202.
8 - Zhong X, Spottiswoode BS, Meyer CH, Kramer CM, Epstein FH. Imaging three‐dimensional myocardial mechanics using navigator‐gated volumetric spiral cine DENSE MRI. Magnetic resonance in medicine. 2010 Oct;64(4):1089-97.
9 - Ennis DB, Nguyen TC, Riboh JC, Wigström L, Harrington KB, Daughters GT, Ingels NB, Miller DC. Myofiber angle distributions in the ovine left ventricle do not conform to computationally optimized predictions. Journal of biomechanics. 2008 Nov 14;41(15):3219-24.
Figures