2097
Visualization of jugular veins from sitting upright to supine position using low field MRI1Magnetic Detection & Imaging, University of Twente, Enschede, Netherlands
Synopsis
Cerebral venous blood takes different pathways depending on body position. Hence, 3D MR imaging of the cervical region at different body inclination angles might give valuable information in patients whose diagnosis relies on imaging of venous pathways. In this study was shown that using a time of flight method the internal jugular veins could be segmented by applying a threshold followed by manual cropping. Subsequently, it was shown that their diameter decreases as the rotational angle is increased towards the upright position. The amount of decrease might give clinically relevant information about the state of the veins and cranial drainage.
Introduction
Previous research has shown that cerebral venous blood takes different pathways depending on body position. In the supine position, cerebral venous drainage is mainly through the internal jugular veins (IJVs), while in the upright position said veins collapse and blood goes primarily through the paravertebral venous plexus1. Hence, upright imaging might give valuable information in patients whose diagnosis relies on imaging of venous pathways that are only activated when upright or whose symptoms differ in the two positions, such as occurs in dural arteriovenous fistulas and idiopathic intracranial hypertension2. Cerebral venous outflow has been previously studied with ultrasound3, but the decrease of flow in the IJVs did not correspond to the flow increase in the venous plexus4. With a rotating low-field MRI scanner, it is possible to study the region of interest (high cervical region) at different degrees of rotation and in 3D.Methods
A 0.25T rotating MRI scanner (Esaote SpA, Genoa, Italy), was used in this study. One healthy volunteer was scanned in the sub-mandibular region, at scanner inclinations of 90° (sitting, analogous to upright), 60°, 30° and 0° (supine position). To gain contrast in the blood vessels a time of flight method was used based on a gradient echo with the following scan parameters: TE/TR = 10/30 ms, flip angle = 75°, FOV=28x28x8 cm³, reconstructed resolution = 1.1x1.1x4 mm³, number of slices = 20. The scan duration was 7 minutes and 50 seconds. The IJVs were segmented from the scans by applying a threshold followed by manual cropping. Subsequently, the diameter was measured at 4 equally separated slices as the mean of the biggest and smallest diameters of the ellipse-shaped cross-sectional areas.Results
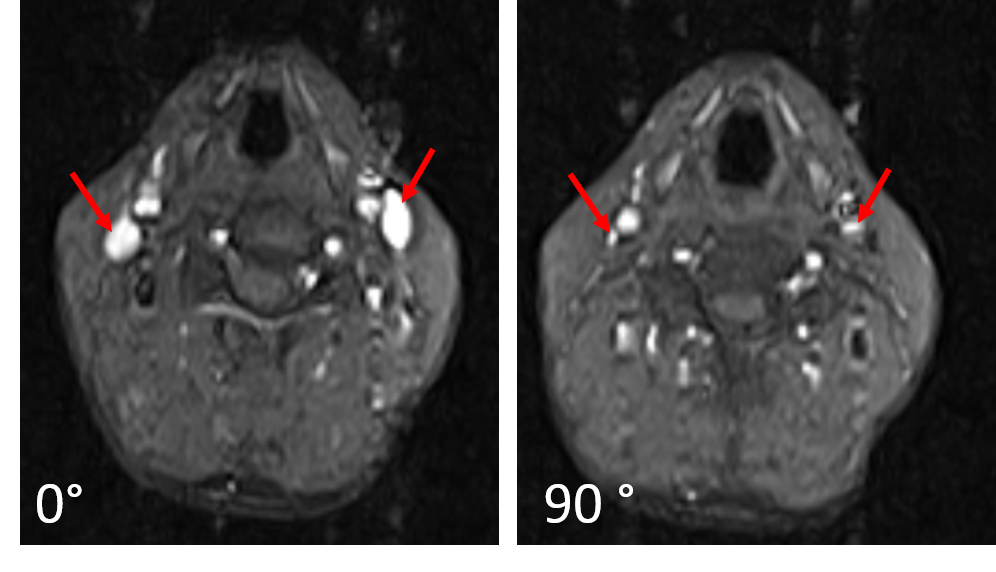
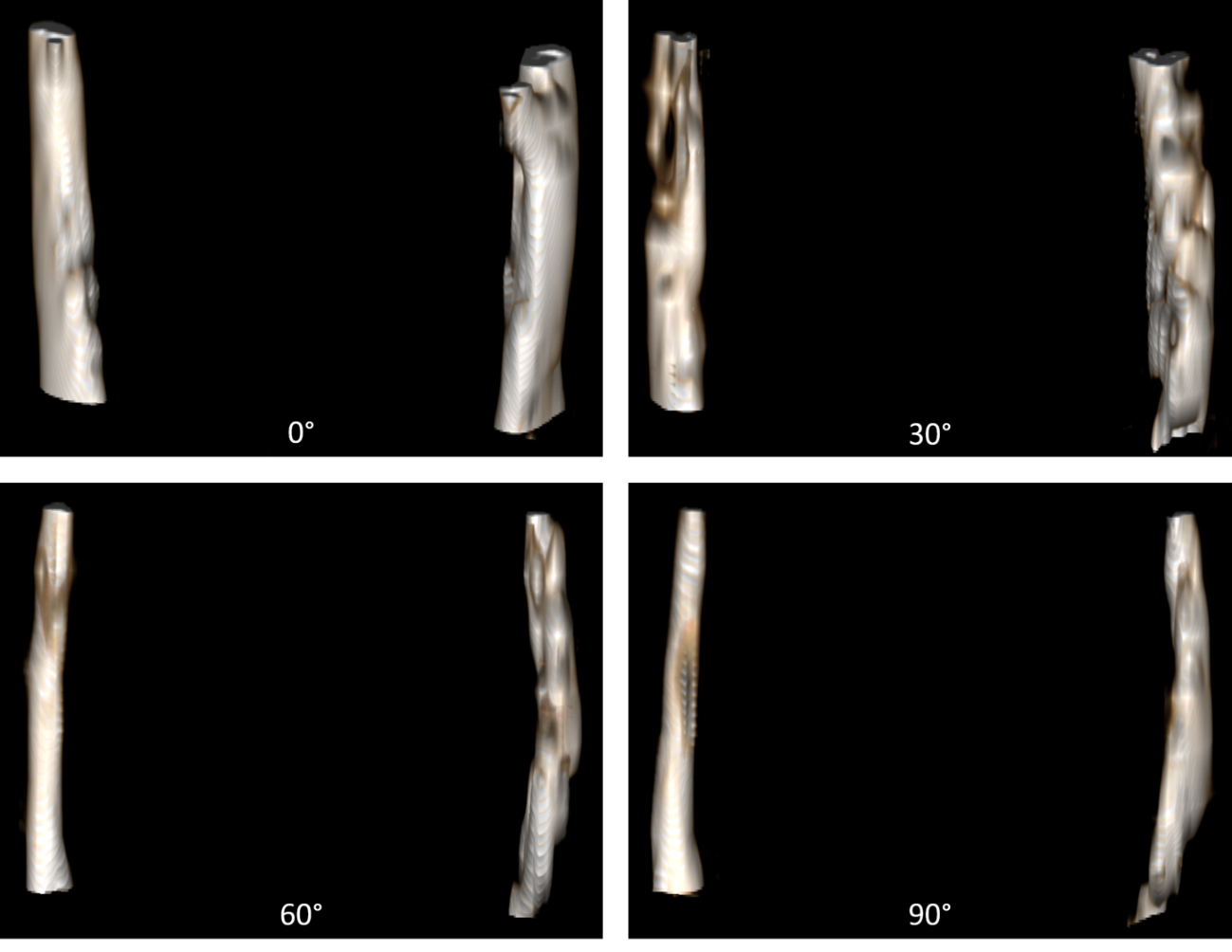
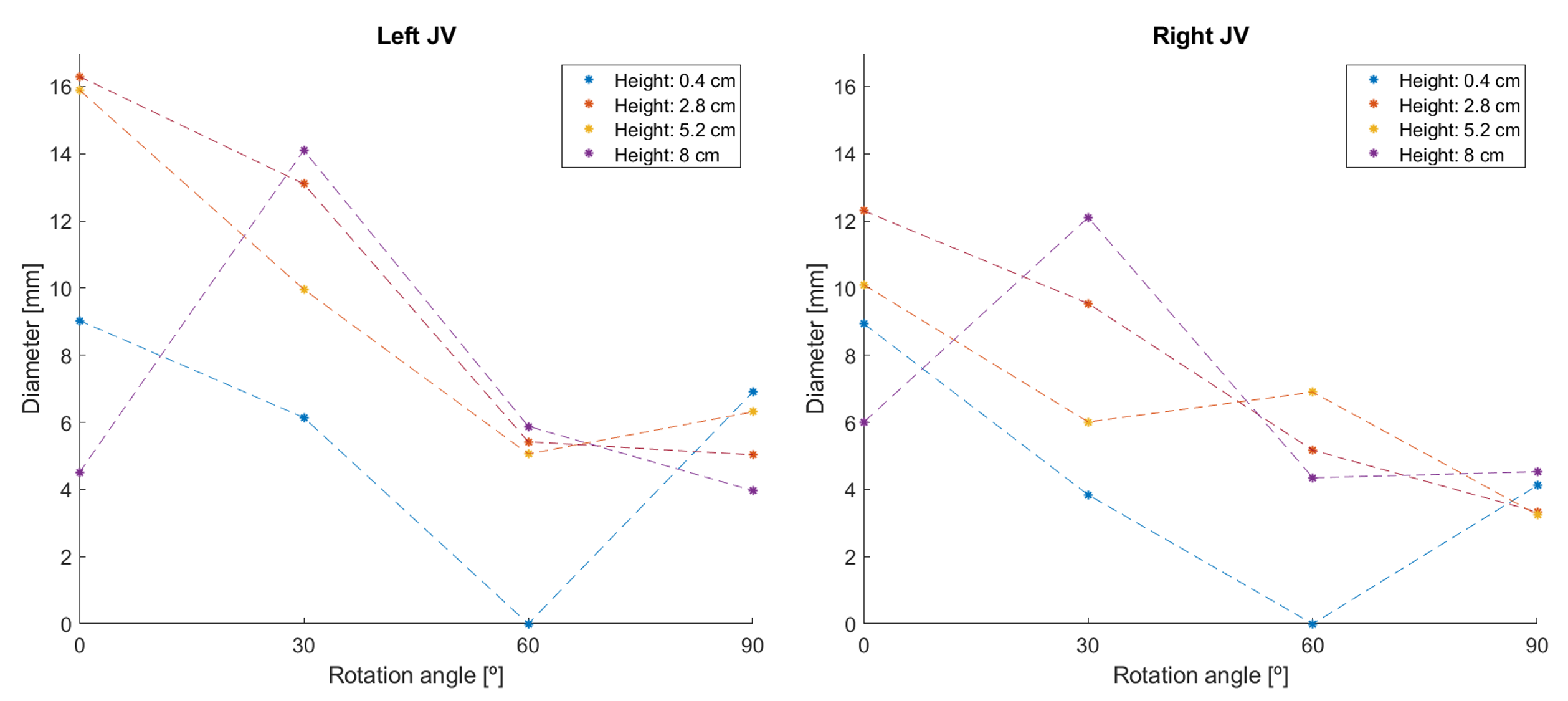
As can be seen in Figure 1, there is a high signal inside the blood vessels opposed to the partly saturated tissue. In the scans made in sitting position the IJVs have a noticeably smaller diameter (maximally 6 and 7 mm) than in supine position (maximally 12 and 16 mm). A complete 3D segmentation of the IJVs in all inclinations can be observed in Figure 2. Although the left IJV is still visible in the upright position, its shape is flattened and less circular. The right IJV is decreased to a smaller diameter than the left one, maintaining a more circular shape. The diameters of the IJVs at different heights were analyzed.Discussion
Conclusion
The IJVs can be effectively be segmented in 3D by lowfield MRI in several inclinations, from supine to the upright position. The amount of decrease in IJV diameter might give clinically relevant information about their condition and cranial drainage.Acknowledgements
No acknowledgement found.References
1. Alperin, N., Lee, S. H., & Bagci, A. M. (2015). MRI measurements of
intracranial pressure in the upright posture: the effect of the hydrostatic
pressure gradient. Journal of Magnetic Resonance Imaging, 42(4),
1158-1163.
2. Qureshi, A. I., Saleem, M. A., Naveed, O.,
Qureshi, M. A., & Wallery, S. S. (2017). Upright Catheter-Based Cerebral
Angiography. Journal of vascular and interventional neurology, 9(6),
14.
3. Valdueza, J. M., von Münster, T., Hoffman, O.,
Schreiber, S., & Einhäupl, K. M. (2000). Postural dependency of the cerebral venous outflow. The lancet, 355(9199),
200-201.
4. Schreiber, S. J., Lurtzing, F., Gotze, R., Doepp, F., Klingebiel, R.,
& Valdueza, J. M. (2003). Extrajugular pathways
of human cerebral venous blood drainage assessed by duplex ultrasound. Journal
of Applied Physiology, 94(5), 1802-1805.
Figures