2095
CrCEST reveals characteristics of skeletal muscle creatine metabolism in patients with Peripheral Arterial DiseaseHelen Sporkin1, Roshin Mathew2, Christopher Kramer2,3, and Craig Meyer1,3
1Biomedical Engineering, University of Virginia, Charlottesville, VA, United States, 2Cardiovascular Imaging, University of Virginia, Charlottesville, VA, United States, 3Radiology and Medical Imaging, University of Virginia, Charlottesville, VA, United States
Synopsis
Peripheral arterial disease (PAD) is an atherosclerotic disease of the limbs. Creatine chemical exchange saturation transfer (CrCEST) MRI can be used to visualize creatine metabolism as it occurs in the muscles of the calf. We have successfully applied CrCEST in 13 healthy subjects and 7 PAD patients in order to characterize the effect of ischemia on skeletal muscle energetics. Creatine concentration decay was assessed by CrCEST over a period of 8 minutes after plantarflexion exercise. Time course CEST asymmetry plots show features of PAD decays that help reveal mechanisms of metabolic dysfunction.
Introduction
Peripheral arterial disease (PAD) is a vascular disease in which arterial atherosclerotic obstructions lead to lower limb ischemia and claudication. PAD affects over 200 million people worldwide, and is the leading cause of lower limb amputation[1]. The current standard PAD imaging method for assessing energetics, 31P magnetic resonance spectroscopy (MRS), suffers from low SNR and requires specialized imaging coils. Creatine chemical exchange saturation transfer (CrCEST) MRI involves selectively saturating amine-bound protons on creatine that are then transferred to free water as creatine metabolism occurs. We have successfully applied CrCEST in 13 healthy subjects and 7 PAD patients in order to characterize the effect of ischemia on skeletal muscle energetics. Creatine concentration decay was assessed by CrCEST over a period of 8 minutes after plantarflexion exercise. Time course CEST asymmetry plots show features of PAD decays that help reveal mechanisms of metabolic dysfunction.Methods
We have applied CrCEST in 16 healthy subjects and 8 PAD patients who performed plantarflexion ergometry to exhaustion or claudication. Creatine levels were measured over 8-10 min using a pulse sequence from the Center for MR and Optical Imaging at the University of Pennsylvania on a Siemens 3T Prisma.[2] Water saturation with shift reference (WASSR) and B1 maps were collected for B0 and B1 correction. Six images were acquired over 24 s intervals with saturation frequency offsets of ±1.3, ±1.8, and ±2.3 ppm. The CEST effect from creatine reduces the signal at +1.8 ppm compared to the reference at -1.8 ppm, referred to as CrCESTasym. A 500 ms saturation pulse train was applied consisting of five 99.6 ms Hanning windowed pulses with 150 Hz B1 amplitude separated by a 0.4 ms inter-pulse delay. A fat saturation pulse was applied, followed by a single-shot spoiled gradient-echo readout with centric encoding, flip angle 10°, FOV 160x160 mm, matrix 128x128, TR 6.0 ms, TE 3 ms, slice thickness 10 mm. An ROI containing the anterior, lateral, and superficial compartments of the calf was drawn by hand for each subject. Values of the mean CrCESTasym signal of the ROI at each acquisition time were fit to a monoexponential with a decay constant τ.Results
Of the 16 healthy volunteers scanned, 3 were excluded due to failure to reach exhaustion within 20 minutes of plantarflexion exercise. The mean τ of the 13 successful in-bore exercise volunteers was 173.5 ± 49.9 s. All 8 PAD patients were able to reach exhaustion, but one was excluded due to severe claudication that required stopping post-exercise imaging. Of the 7 successful scans, 5 showed prolonged decays that were not well defined by an exponential, an example of which is shown in Figure 1. The remaining 2 had a mean τ of 313.3 ± 47.5 s. The shapes of the non-exponential decays varied, but included rises in signal after initially decaying post-exercise.Conclusion
CrCEST shows promise as a useful tool in assessing treatment progress and predicting patient outcomes in patients with PAD. We will continue to recruit more patients in an effort to further characterize creatine decay in PAD. Future work in combining ASL and other CEST metabolites in our protocol will provide a more complete depiction of the effect of PAD on perfusion and metabolism. In particular, a focus on products of anaerobic metabolism will help complement the information given about aerobic metabolism by CrCEST.Acknowledgements
This work was supported by NIH R01 HL 075792 and NIH T32 HL 007284.References
[1] Ostchega, Y, et al. Journal of the American Geriatrics Society 2007; 55: 583-589.
[2] Haris M, et al. Nature Med 2014; 20,2:209-215.
Figures
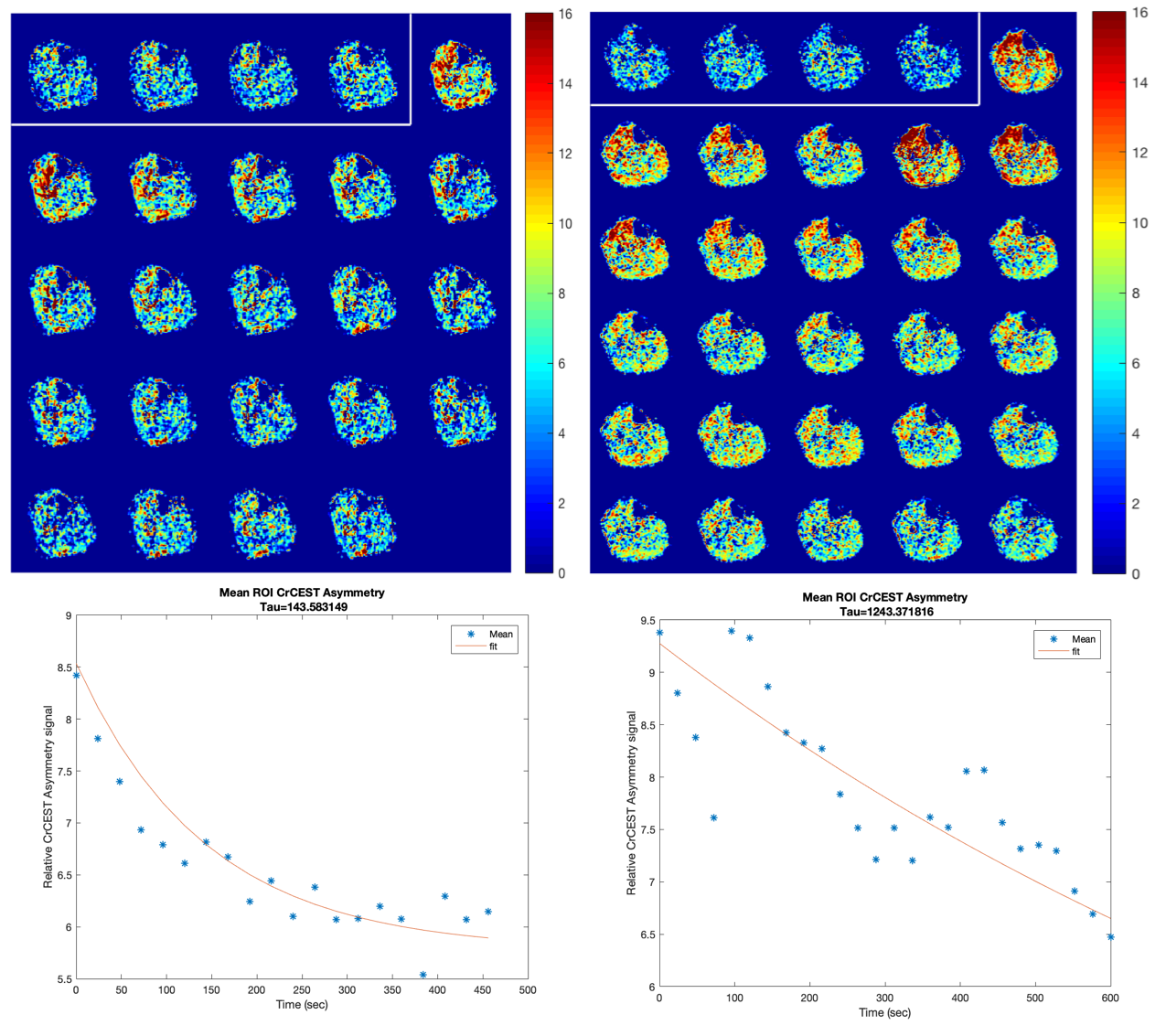
Figure 1: Mean CrCEST Asymmetry decay in a calf muscle ROI of 3 subjects. (left column) CrCEST signal time course (top) and decay (bottom) of a normal age-matched subject. (right column) CrCEST signal time course and decay of a PAD patient with an ABI of 0.74, showing a periodic decay pattern and a poor exponential fit.