2086
Signal-Intensity-Ratio of Carotid Intraplaque Hemorrhage Stratifies Risk of Acute Cerebral Infarct: A Chinese Atherosclerosis Risk Evaluation Study1Department of Radiology, The Affiliated Hospital of Yangzhou University, Yangzhou, China, 2Center for Brain Disorders Research, Capital Medical University and Beijing Institute for Brain Disorders, Beijing, China, 3Department of Radiology, University of Washington, Seattle, WA, United States, 4Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University School of Medicine, Beijing, China
Synopsis
Previous studies have shown that the presence of carotid IPH is a strong predictor for future ischemic events. The present study investigated the usefulness of the signal-intensity-ratio of IPH in carotid arteries for stratification of acute cerebral infarct (ACI) risk using multicontrast MR vessel wall imaging. We found that the signal-intensity-ratio of carotid IPH on T1W images was independently associated with the presence of acute cerebral infarct. Our results suggest that the age of carotid IPH might be an independent indicator for the risk of acute ischemic cerebrovascular events.
Introduction and purpose
Previous studies have shown that presence of carotid intraplaque hemorrhage (IPH) was associated with cerebrovascular ischemic events. 1, 2 Moreover, a recent study by Wang et al reported that plaques on the symptomatic side showed stronger T1 signals compared with those on the asymptomatic side in recently symptomatic patients with bilateral carotid IPH. 3 Currently, mutlicontrast magnetic resonance (MR) vessel wall imaging has been shown to assess the morphological and compositional characteristics of atherosclerotic plaques in carotid artery with high sensitivity and specificity. 4 However, the usefulness of the signal-intensity-ratio (SIR) of carotid IPH on different contrast weightings for risk stratification of acute cerebral infarct (ACI) remains unclear. The objective of the present study was to investigate the association between the SIR of carotid IPH and ACI in patients with hemorrhagic carotid plaques using multi-contrast MR vessel wall imaging.Methods
Study sample: One hundred and eighteen symptomatic patients (mean age, 66.9±10.2 years; 88.1% males) with carotid IPH recruited from a multicenter study of CARE-II (NCT02017756) were included in this study. MR imaging: All patients underwent carotid and brain MR imaging on 3.0T MR scanners (Achieva TX, Philips Healthcare, Best, The Netherlands) with 8-channel phase array carotid coils and head coils. A standardized multisequence protocol was performed for carotid artery by acquiring time-of-flight (TOF), QIR T1-weighted (T1W), MDIR T2-weighted (T2W), and magnetization-prepared rapid acquisition gradient echo (MPRAGE) sequences. Structural MR images of the brain were acquired by scanning T1W and diffusion weighted imaging (DWI) sequences. The imaging parameters are detailed in Table 1. The study protocol was approved by local Ethics Committee at each participating institution and all patients provided written informed consent. Image analysis: The MR images were reviewed by two experienced radiologists with consensus who were blinded to clinical information. IPH was identified by MPRAGE images when hyperintense present (1.5 times of signal intensity compared with muscle). The SIR of carotid IPH against muscle on T1W, T2W, TOF, and MPRAGE images were measured, respectively. The SIR was calculated by dividing the maximum signal intensity of IPH from the mean signal intensity of sternocleidomastoid muscle on each axial image. Presence or absence of ACI was determined on ipsilateral hemisphere to carotid IPH. Statistical analysis: For patients with bilateral carotid IPH, the MR imaging features in plaque with larger plaque burden were selected for analysis. The SIRs of carotid IPH were compared between patients with and without ACI using independent-sample t test or Mann-Whitney U test as appropriate. Logistic regression was utilized to calculate the odds ratio (OR) and corresponding 95% confidence interval (CI) of SIRs of IPH on different imaging sequences in discriminating presence of ACI before and after adjusted for confounding factors.Results
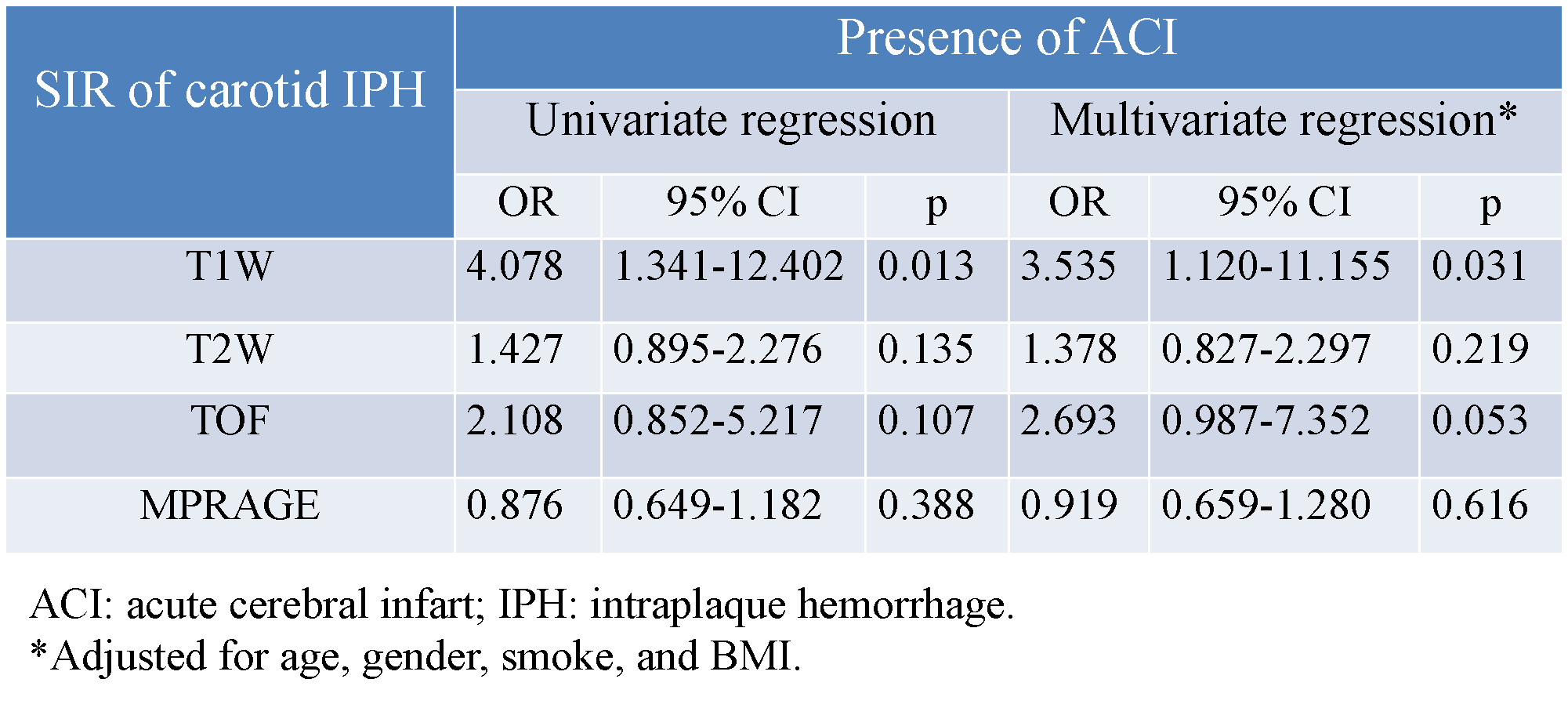
Of 118 included patients, 35.6% had ACI in ipsilateral hemispheres of carotid IPH. Compared with patients without ACI, those with ACI had significantly higher SIRs of carotid IPH on T1W (1.5±0.6 vs. 1.3±0.3; p=0.022) but not on T2W, TOF, and MPRAGE images (all p >0.05, Fig. 1). Logistic regression analysis revealed that the SIR of carotid IPH on T1W images was significantly associated with the presence of ACI before (OR=4.078; 95%CI 1.341-12.402; p=0.013) and after (OR=3.535; 95%CI 1.120-11.155; p=0.031) adjusted for clinical confounding factors (Table 2). No significant association was found between ACI and SIRs on TOF, T2W, and MPRAGE images (all p >0.05). Fig. 2 shows that the patient with higher SIR on T1W images had ACI in the ipsilateral hemisphere on DWI images.Discussion and Conclusion
This study investigated the association of signal-intensity-ratio of carotid IPH against muscle on different MR imaging sequences with acute ischemic infarct. We found that the signal-intensity-ratio of carotid IPH on T1W images was independently associated with the presence of ipsilateral acute cerebral infarct. The signal intensity of IPH is associated with the age of hemorrhage within plaques. High signal intensity of IPH indicates the recent hemorrhage. Our results suggest that the age of carotid IPH might be an independent indicator for the risk of acute ischemic cerebrovascular events..Acknowledgements
We thank all the CARE-II investigators for their contributions to the patient recruitment.References
1. Altaf N, Daniels L, Morgan PS, et al. Detection of intraplaque hemorrhage by magnetic resonance imaging in symptomatic patients with mild to moderate carotid stenosis predicts recurrent neurological events. J Vasc Surg. 2008;47(2):337-342.
2. McNally JS, McLaughlin MS, Hinckley PJ, et al. Intraluminal thrombus, intraplaque hemorrhage, plaque thickness, and current smoking optimally predict carotid stroke. Stroke. 2015;46(1):84-90.
3. Wang X, Sun J, Zhao X, et al. Ipsilateral plaques display higher T1 signals than contralateral plaques in recently symptomatic patients with bilateral carotid intraplaque hemorrhage. Atherosclerosis. 2017;257:78-85.
4. Cai JM, Hatsukami TS, Ferguson MS, et al. Classification of human carotid atherosclerotic lesions with in vivo multicontrast magnetic resonance imaging. Circulation. 2002;106(11):1368-1373.
Figures