2076
Large coverage peripheral artery 3D vessel wall MRI using SUper-Resolution for Psf-Restored Isotropic turbo Spin Echo (3D SURPRISE)1Radiology, University of Washington, Seattle, WA, United States, 2Philips Research North America, Cambridge, MA, United States, 3Surgery, University of Washington, Seattle, WA, United States
Synopsis
Vessel wall MRI for peripheral
artery disease (PAD) atherosclerotic lesions requires large coverage due to
diffuse distribution of lesions, and high-resolution due to smaller plaque
components. However current large coverage PAD approaches uses gradient echo
sequences that may not be optimal for highly calcified PAD lesions. Therefore we
developed and evaluated a large coverage 3D femoral MRI using SUper-Resolution
for Psf-Restored Isotropic turbo Spin Echo
(3D-SURPRISE) that provides shorter scan times with higher SNR and CNR than an existing
large coverage gradient echo femoral vessel wall MRI (3D-MERGE).
Background
PAD is a leading cause of functional disability and morbidity resulting from ischemia of the lower limbs secondary to atherosclerotic plaque deposition in the superficial femoral and popliteal arteries. PAD tends to be diffusely and extensively distributed along the lower limb. Thus, a large coverage vessel wall scan extending from above the common femoral artery bifurcation to the distal lower limb is required for more comprehensive assessment of PAD lesions. While large coverage gradient echo based 3D peripheral artery MRI techniques have been previously described [1,2], they may not be optimal for lesion measurement due to a high percentage of calcified lesions in PAD whose measurements are inflated by susceptibility effects. Therefore, a large coverage high spatial resolution spin echo based vessel wall imaging technique is desirable for PAD MRI. Previous use of variable flip angle fast spin echo sequences for vessel wall imaging have been limited to smaller scan geometries [3]. Moreover, short echo trains are needed for vessel wall imaging to avoid T2 blurring. Scan times may be reduced by using a longer echo train but this strategy requires correction of the point spread function (PSF) to regain actual resolution.Aim
Develop high-resolution large coverage peripheral artery 3D vessel wall MRI using SUper-Resolution for Psf-Restored Isotropic turbo Spin Echo (3D-SURPRISE) and compare vessel wall metrics to 3D gradient echo based PAD vessel wall MRI.Methods
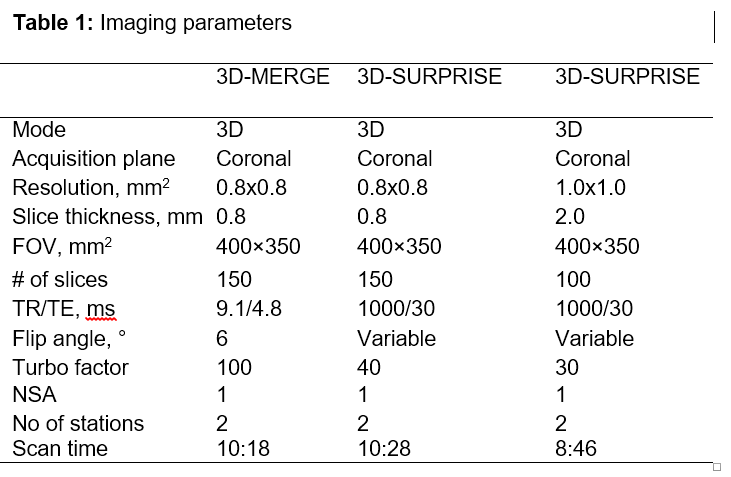
MR scans: Imaging procedures were done under local IRB guidelines and informed consent was obtained from subjects. Two subjects (one normal and one patient with PAD) were scanned on a 3T Philips Ingenia whole body scanner with two phased array torso coils (Philips Healthcare) covering the anterior lower limbs from the groin to the lower leg. These coils were combined with the posterior coils integrated into the scanner bed. 3D SURPRISE: 3D-SURPRISE consists of two components, a 3D large coverage variable flip angle turbo spin echo (VFA TSE) acquisition followed by combined PSF restoration and super-resolution post-processing. Optimization of sequence parameters were done on the normal volunteer. VFA TSE parameters were optimized to match the scan time and resolution of 3D-MERGE [1] (table 1) requiring an echo train length of 40. In order to reduce the scan time further in PAD patients and utilize the super-resolution capability of 3D-SURPRISE, a faster scan with larger voxel size but with shorter echo train of 30 (table 1) was compared in the PAD patient. PSF enhancement and super-resolution processing was applied to the VFA TSE images in the phase and slice encoding directions [4]. Image analysis: Muscle and vessel wall signal-to-noise ratio (SNR) and wall-lumen contrast-to-noise ratio (CNR) were measured separately on 3D-SURPRISE, VFA TSE and 3D-MERGE at ten different locations along the superficial femoral artery (3 in upper thigh, 4 in the adductor canal and 3 in the popliteal). SNR was defined as the ratio of mean signal in the region-of-interest and standard deviation of muscle signal. CNR was defined the difference in mean wall signal and mean lumen signal divided by the standard deviation of muscle signal. 3D-SURPRISE SNR metrics were compared to VFA TSE and 3D-MERGE using paired t-tests (p-value<0.05 was considered statistically significant).Results
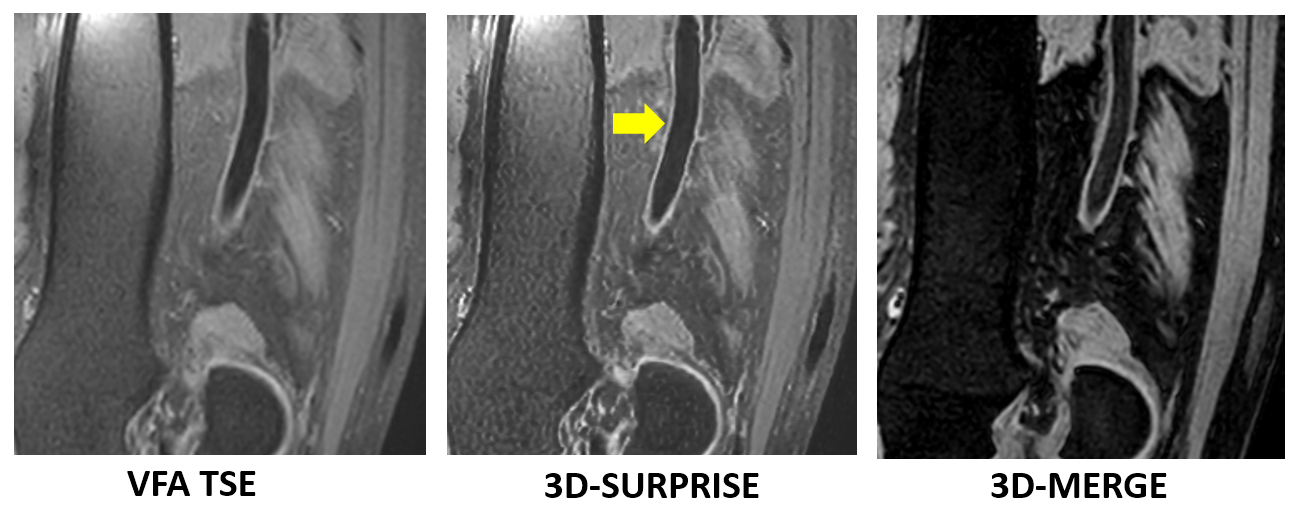
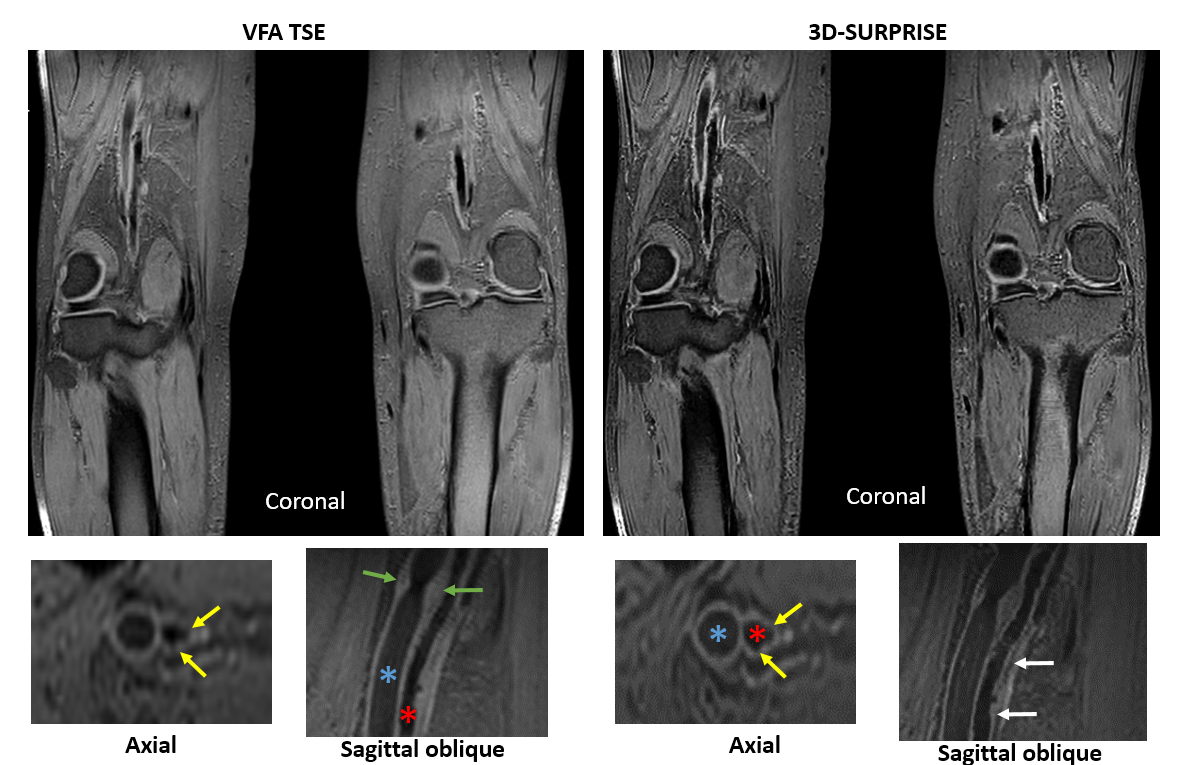
Qualitative comparison showed improved resolution after 3D-SURPRISE processing compared to VFA TSE (figure 1). Outer wall delineation was also improved after 3D-SURPRISE processing compared to 3D-MERGE (figure 1). In PAD lesions, the visibility of small calcifications was improved on 3D-SURPRISE compared to native VFA TSE (figure 2).
Quantitative comparison showed no change in vessel wall SNR or CNR due to 3D SURPRISE processing (table 2). There was a slight decrease in muscle SNR (15.49 ± 4.16 vs 19.46 ± 5.08, p<0.05) after 3D-SURPRISE processing. When compared to 3D-MERGE, 3D-SURPRISE had significantly higher muscle SNR, vessel wall SNR and wall-lumen CNR (all p<0.05, table 2).
Discussion
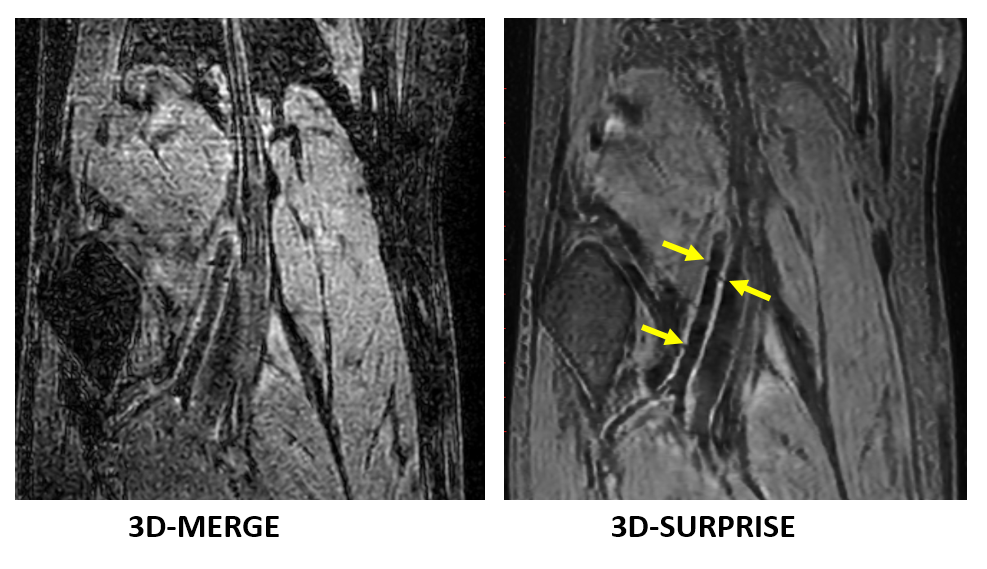
3D-SURPRISE processing of optimized VFA TSE provides large coverage high-resolution PAD vessel wall imaging with shorter scan times and higher SNR than 3D-MERGE. There was a slight decrease in SNR after 3D-SURPRISE processing as shown by decreased muscle signal but it did not affect vessel wall SNR or CNR. 3D-SURPRISE also improved SNR and CNR over 3D-MERGE PAD vessel wall MRI. Initial comparison also shows that the super-resolution processing may also improve the evaluation of small plaque components such as calcification (figure 3).Conclusions
3D-SURPRISE provides large coverage 3D high resolution isotropic PAD vessel wall MRI with higher SNR and CNR than 3D-MERGE PAD vessel wall MRI, in a shorter scan time.Acknowledgements
This work was partially supported by NIH grant R01HL103609.References
[1] Chiu B, Sun J, Zhao X, Wang J, Balu N, Chi J, Xu J, Yuan C, Kerwin WS., Fast plaque burden assessment of the femoral artery using 3D black-blood MRI and automated segmentation, Med Phys. 2011 Oct;38(10):5370-84. doi: 10.1118/1.3633899.
[2] Xie G, Zhang N, Xie Y, Nguyen C, Deng Z, Bi X, Fan Z, Liu X, Li D, Fan Z, DANTE-prepared three-dimensional FLASH: A fast isotropic-resolution MR approach to morphological evaluation of the peripheral arterial wall at 3 Tesla, J Magn Reson Imaging. 2016 Feb;43(2):343-51. doi: 10.1002/jmri.24986.
[3] Zhang Z, Fan Z, Carroll TJ, Chung Y, Weale P, Jerecic R, Li D, Three-dimensional T2-weighted MRI of the human femoral arterial vessel wall at 3.0 Tesla, Invest Radiol. 2009 Sep;44(9):619-26. doi: 10.1097/RLI.0b013e3181b4c218.
[4] Zhou Z, Chen S, Wu J, Zhao X, Börnert P, Yuan C, Deep Convolutional Neural Network Enhanced 3D High Resolution Turbo Spin Echo Intracranial Vessel Wall Imaging, ISMRM 2018.
Figures