2074
Quantitative measurements of decreased arterial collateralization and branching in peripheral artery disease.1Radiology, University of Washington, Seattle, WA, United States, 2Electrical Engineering, University of Washington, Seattle, WA, United States, 3University of California SanFrancisco, San Francisco, CA, United States, 4Surgery, University of Washington, Seattle, WA, United States
Synopsis
The extent of collateralization/branching
(CB) of lower limb vessels in peripheral artery disease (PAD) can inform risk
of ischemia and response to revascularization. However quantitative imaging
metrics of CB have not been assessed in the setting of severe PAD. We developed
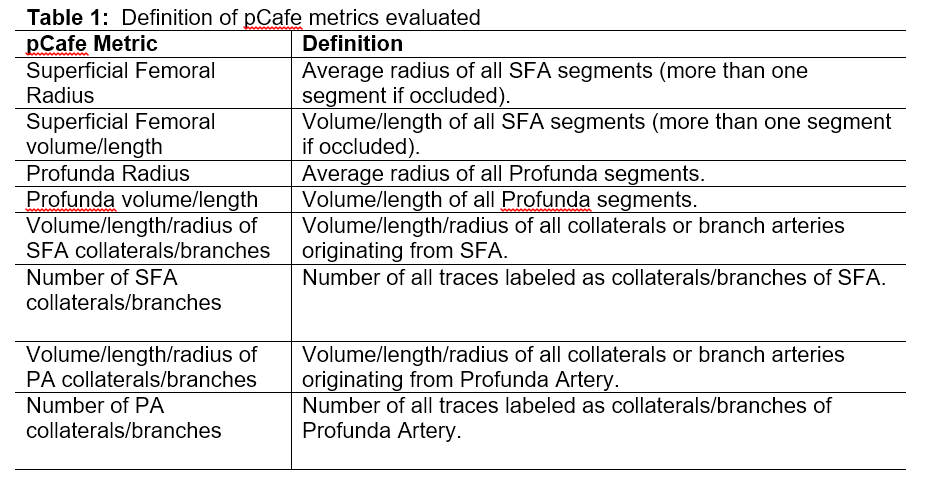
automated quantitative measurements of lower limb vascular morphology (pCafe)
and compared CB in patients undergoing revascularization for PAD. Assessment of
pCafe metrics in severe PAD suggests CB is increased with occlusion compared to
stenosis indicating compensatory CB development.
Background
PAD due to atherosclerosis of the superficial femoral artery (SFA) can cause limb threating ischemia. However, the extent of collateralization/branching (CB) can ameliorate the symptoms [1] and also determine the success of revascularization procedures. Therefore, knowledge of the individual patient’s CB can help stratify ischemia risk and guide revascularization/treatments. However quantitative imaging measurements of CB and its effects in severe PAD are limited [1]. The aim of this study is to compare CB in different degrees of SFA patency using an automated quantitative measurement of lower limb vessel morphology.Methods
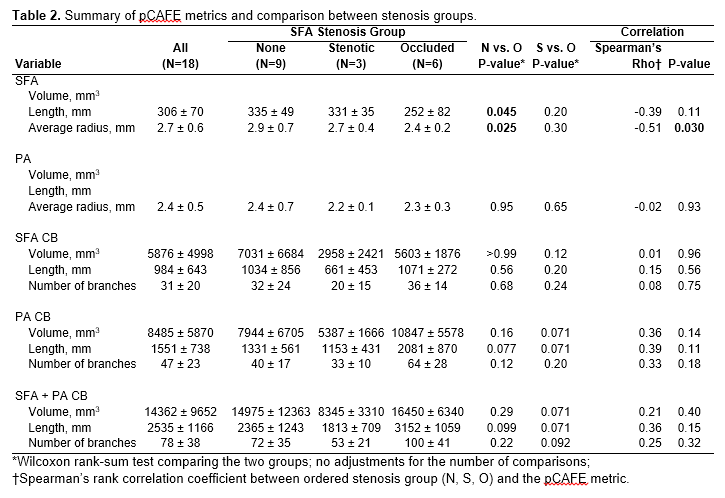
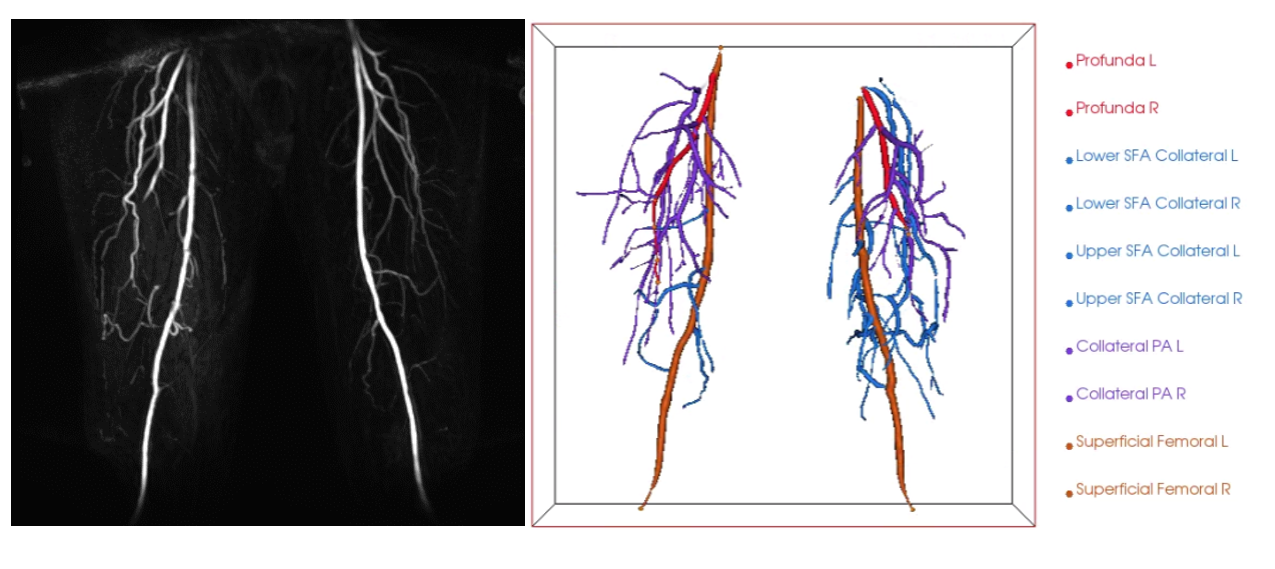
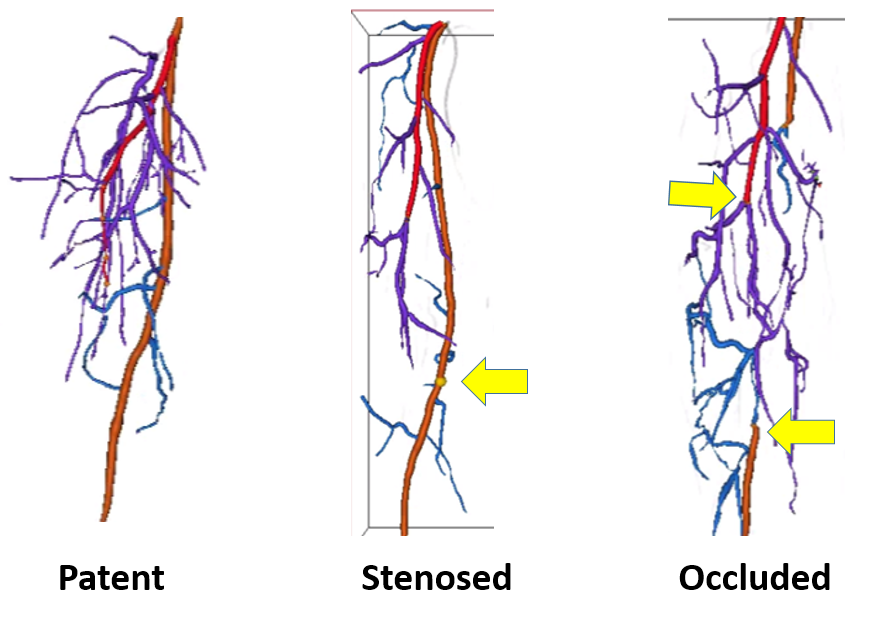
Study subjects and procedures: Ten patients with peripheral artery disease (PAD) scheduled for lower extremity endovascular reconstruction were recruited at two different institutions. Imaging procedures followed institutional IRB guidelines and informed consent was obtained from subjects prior to the scan. MRI scans: Subjects were scanned on either 3T Siemens Skyra or Philips 3T Ingenia scanners. Single station first pass 3D CEMRA was obtained after single dose gadolinium contrast injection (Prohance or Gadavist) covering the lower thigh and knee bilaterally using surface phased array coils. Similar scan parameters were used on both platforms, namely: TR/TE = 4.56/2.195 ms, flip angle = 20°, in-plane resolution = 0.81 mm×0.81 mm, slice thickness = 3 mm, field of view = 430 mm*430 mm. Collateral and branch artery quantification: One subject was excluded due to insufficient image quality. Peripheral arterial feature extraction (pCafe) was based on centerline tracing [2]. Briefly, CEMRA was resampled to 0.81 mm isotropic resolution followed by Nyul intensity normalization [3] and arterial centerline tracing [4]. An expert reader then labeled key landmark points of major arteries namely superficial femoral artery (SFA) and profunda femoris (PA). In cases of SFA stenosis, the site of stenosis was labeled. In cases of SFA occlusion, proximal and distal SFA segments were labeled (distal labeled if present). Arterial branches besides the SFA and PA segments were then automatically labeled as collaterals/branches (CB) (figure 1). Both collaterals and branches were included in this category since the intent was to examine whether total branches distal to occlusion/stenosis was increased. Based on the centerlines and labels, length, radius and number of branches of each segment were automatically calculated (list provided in table 1). Statistical analysis: Arteries from each leg (18 legs in total) were considered separately. Based on SFA patency on the original CEMRA, lower limbs were classified into those with no-stenosis, stenosed or occluded SFA. Representative examples of each type are shown in figure 2. Each of the pCafe metrics was compared using Spearman’s rank correlation coefficient between ordered stenosis group (None, Stenosis, Occluded). Wilcoxon rank-sum test was used to compare the no-stenosis and occluded arteries. P-values less than 0.05 were considered statistically significant.Results
Collateral/branch quantification was achieved in all cases. There was marked individual variation in collateral/branch appearances. There were statistically significant differences in SFA length and average radius between the three groups with decreased length and radius in occluded arteries compared to arteries with no stenosis (length 335 ± 49 mm vs 252 ± 82 mm, p<0.05; radius 2.9 ± 0.7 vs 2.4 ± 0.2 mm, p<0.05). Comparing arteries with stenosis and occlusions, we found a trend towards increased volume, length and number of branches in CB in both SFA and PA when the artery was occluded as opposed to those with only stenosis (table 2).Discussion
pCafe metrics showed decreased SFA length and radius as expected in patent SFA compared to SFA with stenosis. There was a trend for increased CB (length, radius and number of branches) in legs with occluded SFA when compared to limbs with stenosis. With chronic occlusion, collateralization is known to increase. pCafe metrics also show this to be the case and the increased CB in these cases suggest that these limbs may be at lower risk of functional impairment. This is the first study to compare objective quantitative measurements of lower limb CB for stratification of stenosis and occlusion. Our sample size was restricted due to the specific type of patients recruited (PAD subjects scheduled for revascularization). Due to the small sample sizes, standard statistical methods which treat all observations as independent were used (e.g., Wilcoxon rank-sum test, Spearman’s rank correlation). Additional subject inclusion will also help to study patient level differences in collateralization/perfusion using iCafe metrics and relation to patient symptoms.Conclusions
In PAD with compromised SFA (stenosis/occlusion) there was a trend towards increased CB with occlusion compared to stenosis. Our results suggest that CB quantification by pCafe may be useful in stratification of perfusion to lower limb tissues in PAD.Acknowledgements
This work was partially supported by grants from R01HL128816, R01HL103609 and R01NS092207References
[1] McDermott MM, Carr J, Liu K, Kramer CM, Yuan C, Tian L, Criqui MH, Guralnik JM, Ferrucci L, Zhao L, Xu D, Kibbe M, Berry J, Carroll TJ., Collateral vessel number, plaque burden, and functional decline in peripheral artery disease., Vasc Med. 2014 Aug;19(4):281-288. Epub 2014 Jul 21.
[2] Chen L, Mossa-Basha M, Balu N, et al. Development of a quantitative intracranial vascular features extraction tool on 3D MRA using semiautomated open-curve active contour vessel tracing. Magn Reson Med. 2018;79(6):3229-3238. doi:10.1002/mrm.26961.
[3] Nyul LG, Udupa JK, Zhang X. New variants of a method of MRI scale standardization. IEEE Trans Med Imaging. 2000;19(2):143-150. doi:10.1109/42.836373.
[4] Wang Y, Narayanaswamy A, Tsai CL, Roysam B. A broadly applicable 3-D neuron tracing method based on open-curve snake. Neuroinformatics. 2011;9(2-3):193-217. doi:10.1007/s12021-011-9110-5.
Figures