2071
Dynamic MRI visualization of the brachial artery during upper arm air cuff inflations1MR Clinical Science, Philips Healthcare, Best, Netherlands, 2Philips Research, Eindhoven, Netherlands, 3Department of Electrical Engineering, Eindhoven University of Technology, Eindhoven, Netherlands
Synopsis
We investigated the feasibility of imaging the upper arm using real-time and cine MRI during air cuff inflations in order to characterize the elastic properties of the brachial artery. Both the cine, as well as the real-time MR image data allow the direct observation of the occlusion and re-opening of veins and arteries as a function of cuff pressure. They could therefore be potentialy well suited to estimate the elastic properties of the brachial artery, e.g. the area-pressure curve, in vivo. Furthermore, the MR data allow observing the compression and displacement of arm tissue with the future aim to validate and extend existing models of the auscultatory and oscillometric blood pressure measurements.
Introduction
The predominant methods in non-invasive blood pressure measurements are the auscultatory technique and oscillometric technique. Both rely on an initial near complete occlusion of the brachial artery, achieved by inflating an upper arm air cuff to supra-systolic pressure (180mmHg). As the air cuff pressure is released, the blood flow through the artery commences again during those phases of the cardiac cycle where the central blood pressure over-powers the occlusive force of the arm cuff. As the cuff pressure drops below the diastolic blood pressure, the blood flow through the brachial artery is unhindered again. This process is accompanied by characteristic Korotkoff sounds, used in the auscultatory technique, and cuff pressure oscillations used in the oscillometric technique. The underlying fluid mechanical processes are not completely understood, largely because they are difficult to observe directly. Consequently, they have attracted great scientific interest for a long time [1]. In this line of research, a central part is characterization of the elastic properties of the brachial artery, which also has diagnostic value in itself [2]. The elastic properties of the artery are often described by the area-pressure (AP) curve which shows the dependency of the arterial lumen area on the transmural pressure. Other studies reported on brachial artery mechanics measurements using ultrasound [3], [4]. We investigated the feasibility of estimating the lumen area of the brachial artery during pressure cuff inflation using dynamic MRI.Methods
We scanned three volunteers; the first two volunteers were used to optimize the coil setup and imaging protocols. One volunteer was used to acquire MR images during a total of five complete arm cuff pressurizations. Three continuous inflation-deflation cycles were imaged with a high temporal resolution real-time scan and two stepped inflations at cuff pressures of 0, 25, 50, 75, 100, 125, 150 and 175 mmHg were imaged with a high spatial resolution multi-phase scan. The cuff pressurization was performed using a hand-operated BoSo Aneroid Sphygmomanometer placed outside the MRI scanner room and connected via a 20-meter long SMC pneumatic polyurethane air tube with 6 mm outer and 4 mm inner diameter through the waveguide to a MR compatible disposable Philips cuff. All experiments were performed on a Philips Ingenia 1.5T with standard dStream anterior and posterior body coils. Imaging parameters of the high temporal resolution real-time bSSFP scan were TE/TR = 1.6/3.2 ms, 50 degrees flip angle, 300x300 mm FOV and 1.5x1.5x10 mm voxel size. A compressedSENSE factor of 3 was used to obtain 5 frames per second. The high spatial resolution scan was a retrospective cardiac triggered bSSFP cine with 9 cardiac phases,TE/TR = 2.3/4.6 ms, 60 degrees flip angle, 0.7x0.7x8 mm voxel size and SENSE factor 2, resulting in a scan time of 16 seconds.Results
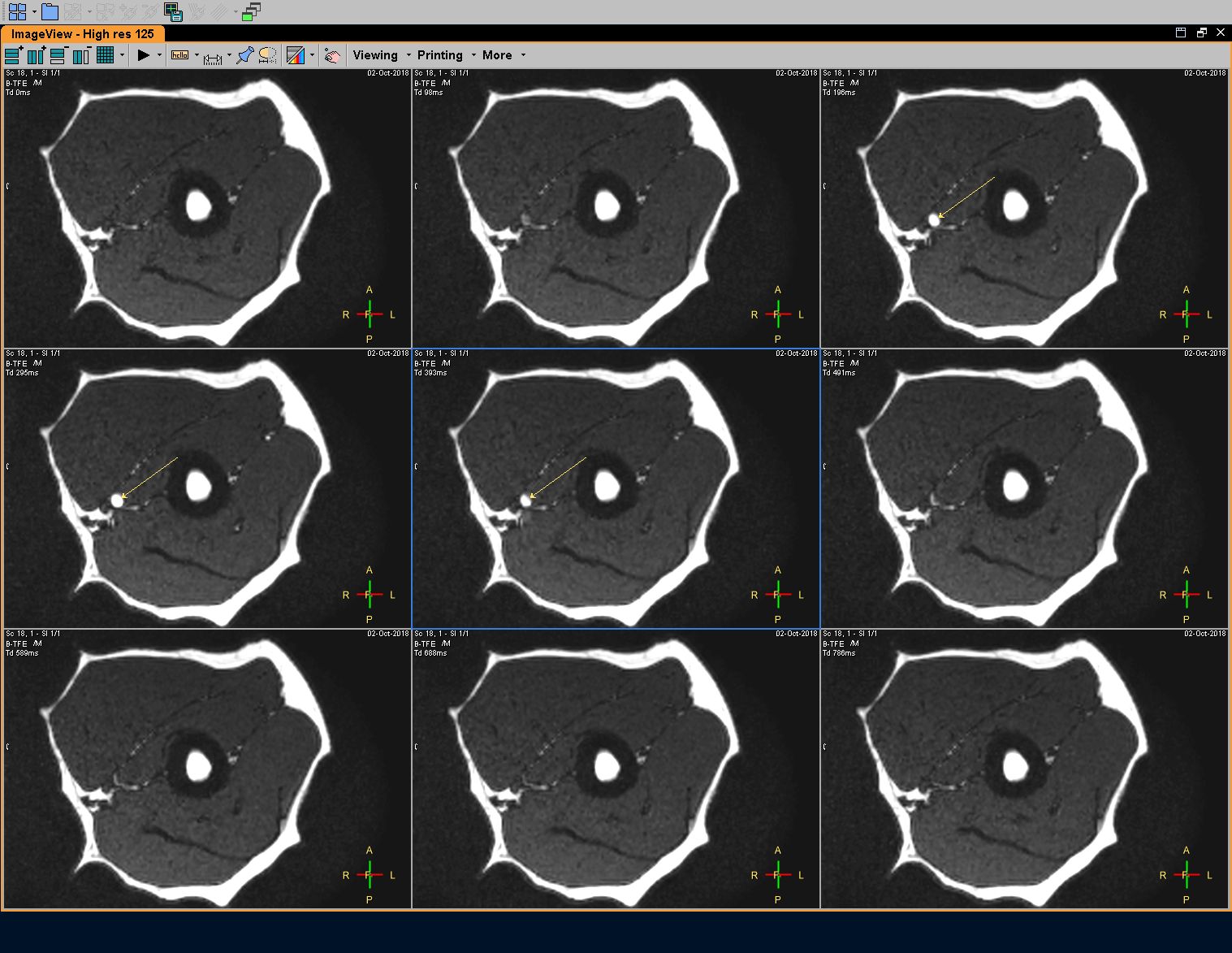
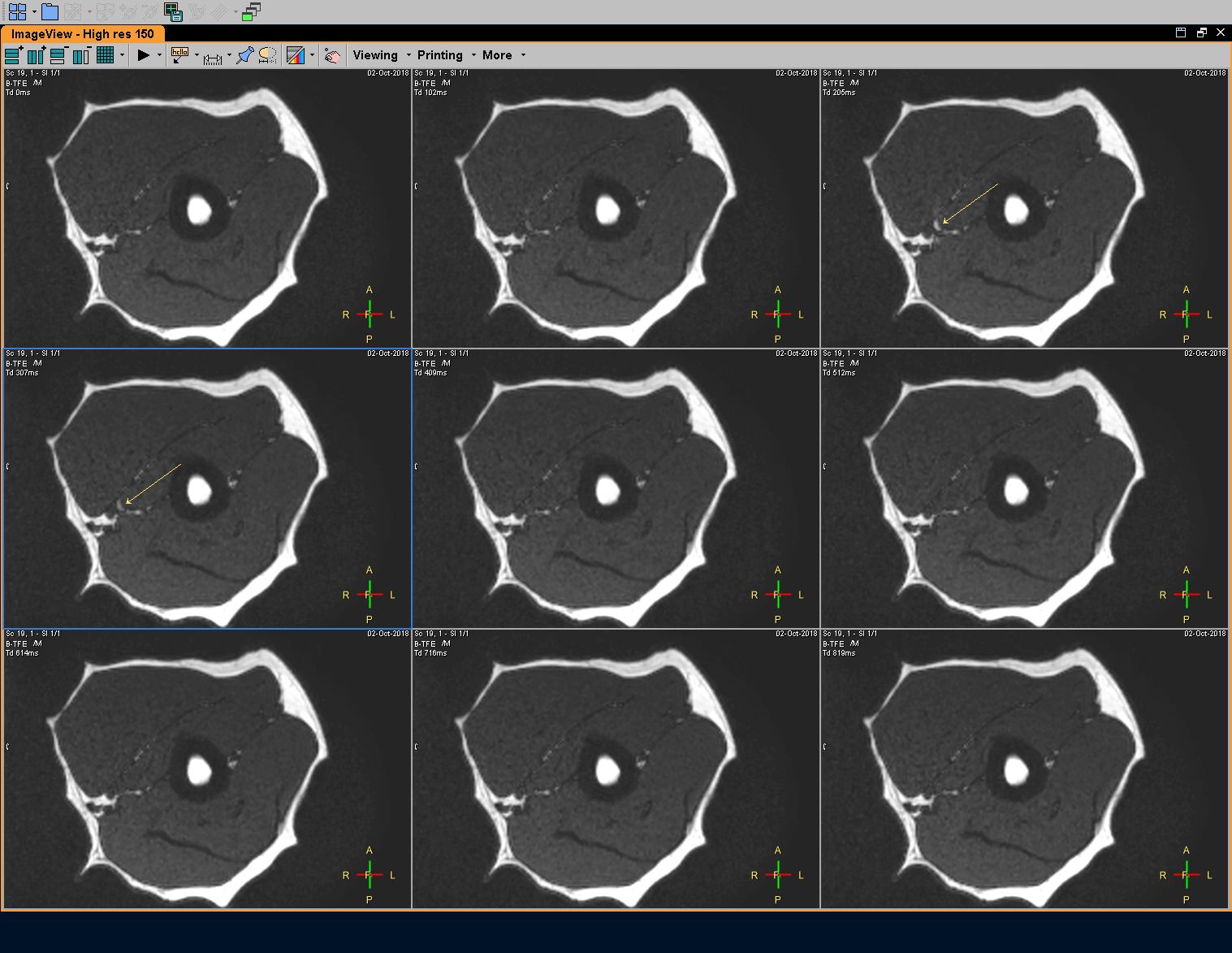
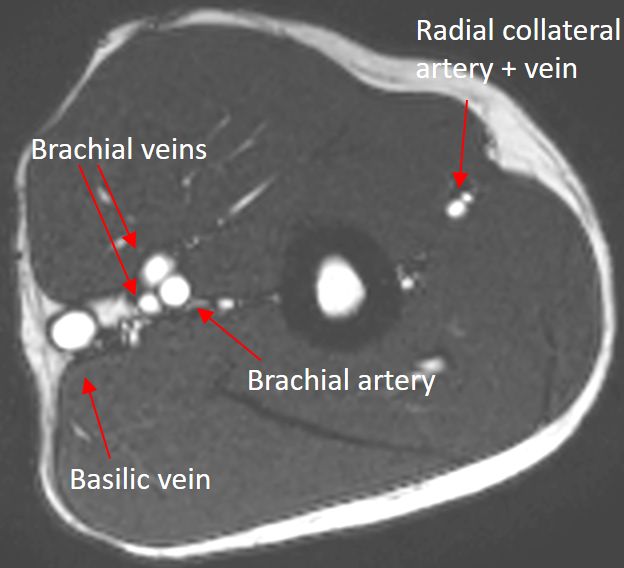
MR Imaging during cuff pressurizations did not cause any patient discomfort. The anterior coil provided enough space to place and inflate the cuff. The cuff was made entirely out of MR-compatible material and did not cause image artefacts. Arteries and veins could clearly be identified as shown in Figure 1. Real-time MRI and cuff pressures during the continuous inflation to 180 mmHg within 15 seconds are shown in figure 2. At 8 seconds, the first closing of the artery is seen and at 9.3 seconds, the last opening is seen. Approximately, these time points correspond to the diastolic pressure at 111 mmHg and systolic pressure at 134 mmHg respectively. Figure 3 shows the nine phases at 125 and Figure 4 at 150 mmHg. At 125 mmHg, the artery opens in phase 3-5. At 150 mmHg, even though this is above systolic pressure, there is a minimum opening of the artery seen in phases 3 and 4. During both continuous and stepped pressure profiles, the pressure signal observed on the sphygmomanometer through the 20m tube appeared to be of good enough quality to allow blood pressure estimates of the subject.Discussion and conclusion
To the best of our knowledge, this is the first case report of real-time MR imaging of the brachial artery during cuff inflation. Both the cine, as well as the real-time MR image data allow the direct observation of the occlusion and re-opening of veins and arteries as a function of pressure. They are therefore promising imaging techniques to estimate the AP-curve of the brachial artery in vivo. Furthermore, the MR data allow to observe the compression and displacement of arm tissue, and the shaping of the arm-cuff interface under the cuff, with the future aim to validate and extend existing models of the auscultatory and oscillometric blood pressure measurement techniques.Acknowledgements
No acknowledgement found.References
1. Drzewiecki, G., Hood, R., & Apple, H. Theory of the oscillometric maximum and the systolic and diastolic detection ratios. Annals of biomedical engineering, 22(1), 88-96, 1994
2. Mackenzie, I. S., Wilkinson, I. B., & Cockcroft, J. R. Assessment of arterial stiffness in clinical practice. Qjm, 95(2), 67-74, 2002
3. Bank AJ, Kaiser DR, Rajala S, Cheng A. In vivo human brachial artery elastic mechanics: effects of smooth muscle relaxation. Circulation 41-7, 1999.
4. Wiesmann F, Petersen SE et al. Global impairment of brachial, carotid, and aortic vascular function in young smokers: Direct quantification by high-resolution magnetic resonance imaging JACC 44-10, 2004.
Figures
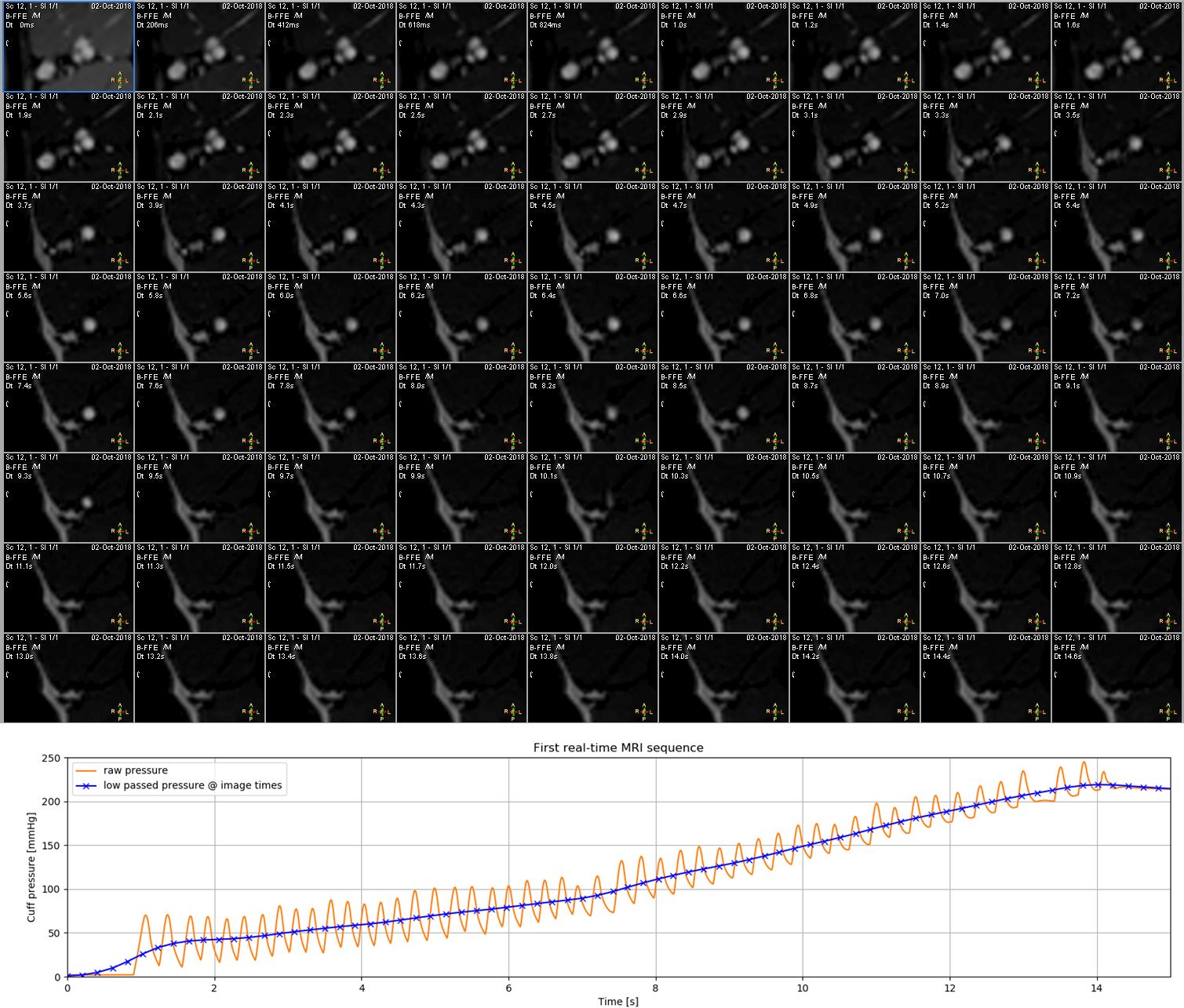
Top: Real-time b-FFE scan, zoomed-in on the brachial artery and veins and the basilic vein with a temporal resolution 206 ms. Closing of the basilic veins starts at 2.5 s (approx. 45 mmHg) and and is complete at 4.9 s (approx. 69 mmHg). The first closing of the brachial artery is seen at 8.0 s (approx. 111 mmHg) and the last opening at 9.3 s (approx. 134 mmHg).
Bottom: recording of the cuff pressure during the real-time scan showing the raw pressure signal in orange and in blue the low-pass filtered pressure with "x" indicating the dynamic scan times.