2069
Initial Study on Coronary MRI at 3T in the Presence of Resorbable Magnesium Scaffolds1Department of Radiology, Medical Physics, Medical Center University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany, 2Department of Cardiology and Angiology I, Heart Center Freiburg University, Faculty of Medicine, University of Freiburg, Freiburg, Germany
Synopsis
Coronary MRI allows for the assessment of vascular patency and thus is a desirable imaging tool for the follow-up of vascular patency after percutaneous coronary interventions in which stenosis are treated with stents. We show that, coronary MR in the presence of recently introduced resorbable magnesium scaffold seems not feasible for the detection of in-stent restenosis within the first year post-intervention as signal voids caused by the scaffold may be miss-interpreted as stenosis. However, coronary MRI provides a valuable tool to further study the resorption process of magnesium scaffolds and to visualize the artery after complete resorption of the scaffold.
Introduction
Coronary MRI allows for the assessment of vascular patency and detection of stenoses in patients with coronary artery disease1. Furthermore, coronary MRI is a desirable imaging tool for the follow-up of vascular patency after percutaneous coronary interventions in which stenosis are treated with stents. Conventional drug eluting metallic stents do not allow for imaging of the stented lumen2 whereas bioresorbable vascular scaffolds made from poly-lactate enable artifact-free imaging of the scaffolded lumen3. Recently, a new type of resorbable scaffold has been introduced that consists of a magnesium-alloy backbone4. In this study, we show initial results of in vivo 3T coronary MRI in the presence of magnesium scaffolds. In addition, potential changes in imaging artifacts that occur due to the resorption of the magnesium backbone are assessed by a one-year follow-upMethods
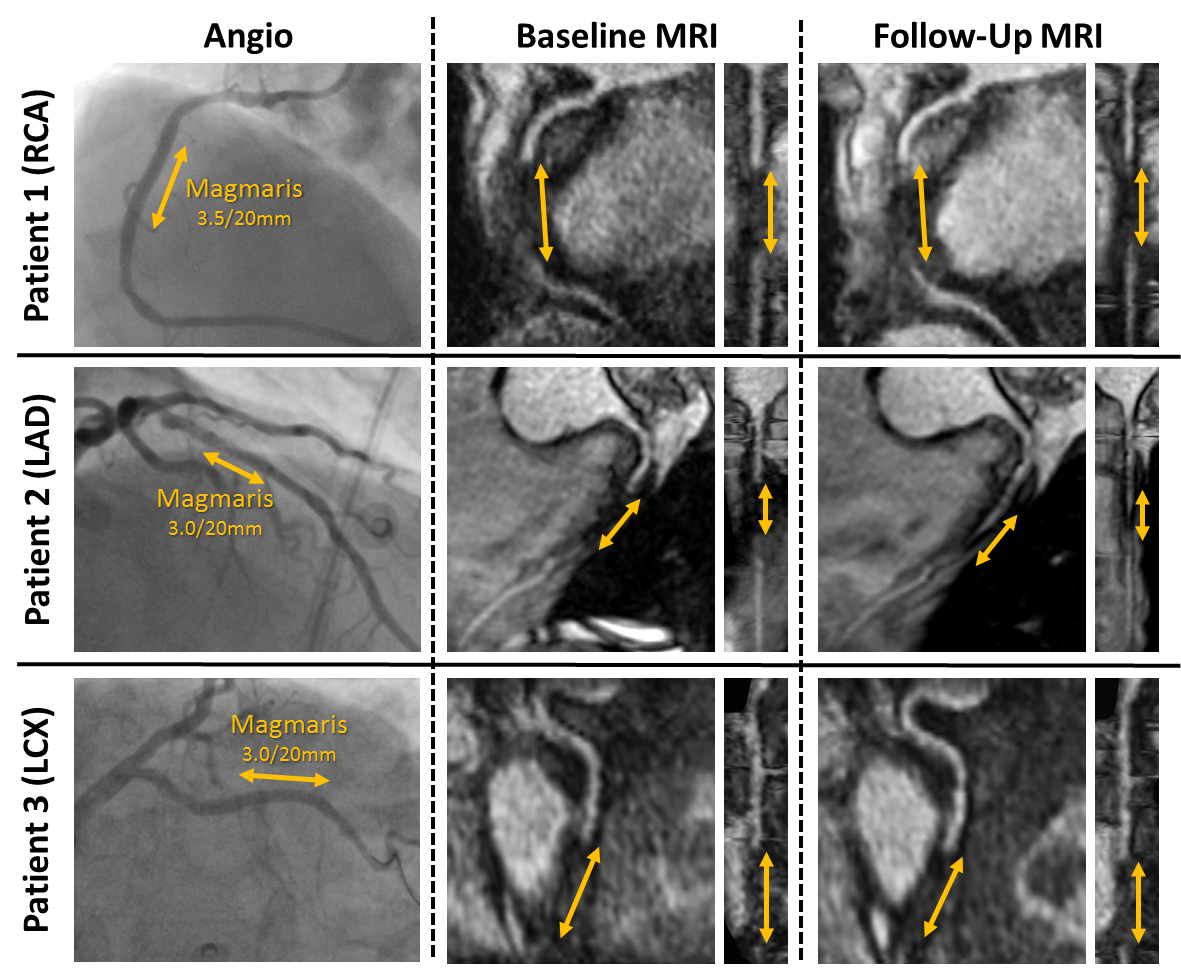
Three patients were included that received a magnesium scaffold (Magmaris, Biotronik AG, Buelach, Switzerland) in proximal segments of the LAD, LCX and RCA. Baseline MR exams were performed within three days post-intervention and all patients were imaged again after 12 months with the same protocol.
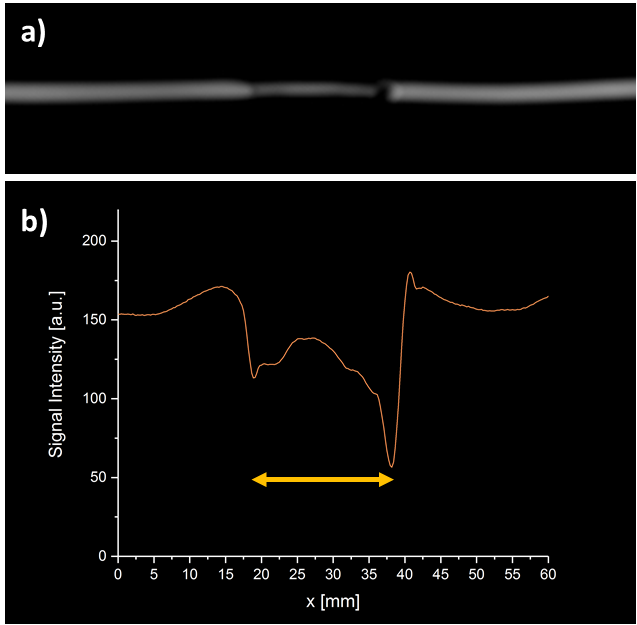
All MR images were acquired using ECG triggering and 3D acquisitions were gated to end-expiration. No contrast agent was used. Coronary arteries were localized using a whole-heart low-resolution 3D-bSSFP sequence with fat-saturation. This was followed by a 3D bright-blood navigator-gated FLASH sequence with 1.08 mm isotropic resolution, fat-saturation and T2-preparation (TE/TR: 1.9/3.1 ms, FoV: 28x277x295 mm³, TET2prep: 40 ms, R=2). The same sequence was used for in vitro imaging of a magnesium scaffold (diameter: 3mm, length: 20 mm) placed in a plastic tube filled with water, which was positioned 45° to B0 for a realistic geometrical configuration.
3D datasets of the coronary arteries were reformatted using IMPAX (AGFA Healthcare). Straightened projections of the arteries were reconstructed using the same software to measure the signal along the scaffolded artery.
Results
Fig.1 shows imaging results of three patients for both the baseline and follow-up exam as well as angiography images. In the initial exam a signal void within the lumen at the location of the scaffolds is seen for all three patients. However, surrounding tissue is not affected by the artifacts. The same signal void is observed in the follow-up exam in patients 1 and 3, but not for patient 2. Here, the signal void is substantially reduced in the proximal part of the scaffolded segment whereas the distal part is still obscured by a weak artifact.
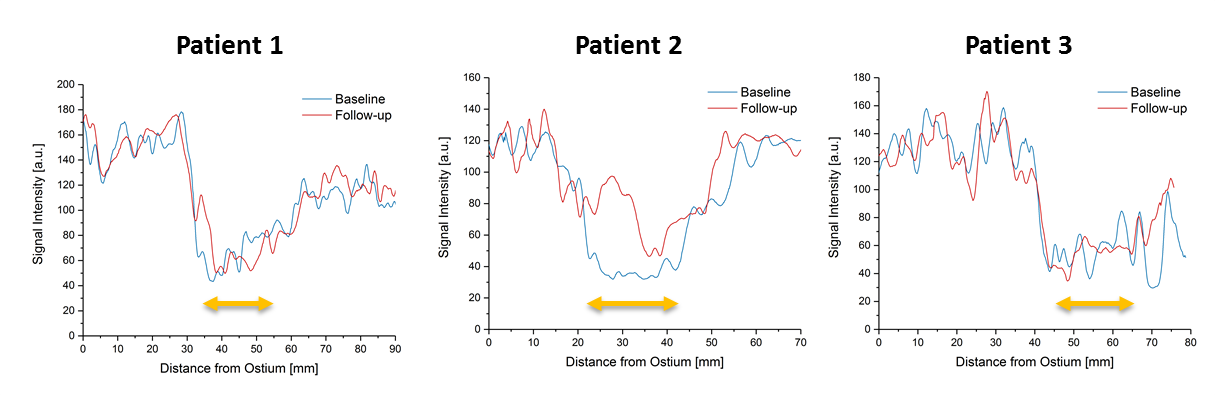
Fig.2 shows the luminal signals along the scaffolded arteries for all three patients and both the baseline and follow-up exam. In the initial exam a signal decrease of about 65% within the scaffolded lumen compared to the signal measured proximally and distally to the scaffold position is measured. A similar signal decrease is observed in the follow-up for patients 1 and 3. For patient 2, the signal decrease is reduced to 31%.
Fig.3 shows the in vitro image acquired with the scaffold placed in a tube. Here, the scaffold causes a minor signal void at the tube walls and the center of the lumen is still visible. However, a signal decrease of 32% is also observed at the center.
Discussion & Conclusion
In vitro imaging results show that, magnesium scaffolds cause only minor artifacts, which are associated with susceptibility induced dephasing in the vicinity of the scaffold. However, due to the limited spatial resolution in coronary MRI, this artifact causes a substantial decrease of the observed luminal signal in the center of the artery. In the in vivo scenario, this leads to a decrease of the luminal signal to below the noise level such that the artery cannot be visualized within the scaffolded segment. Invasive imaging studies have shown, that the magnesium backbone decreases in size and gets converted to calcium phosphate during the resorption process5. As magnesium is paramagnetic whereas calcium phosphate is diamagnetic6, a decrease of the size of the susceptibility artifact via the conversion is expected. In addition, the reduction of the amount of material, i.e. the backbone, will also lead to a reduced artifact. However, the time course of the resorption process differs between patients, which correlates to the mixed findings in the follow-up of our study. Here, in one of three cases a substantial reduction of the scaffold artifact is observed after one year.
In summary, coronary MR in the presence of resorbable magnesium scaffold seems not feasible for the detection of in-stent restenosis within the first year post-intervention as signal voids caused by the scaffold may be miss-interpreted as stenosis. However, coronary MRI provides a valuable tool to further study the resorption process of magnesium scaffolds and to visualize the artery after complete resorption of the scaffold.
Acknowledgements
No acknowledgement found.References
1. Kim WY, Danias PG, Stuber M, et al. Coronary Magnetic Resonance Angiography for the Detection of Coronary Stenoses. N. Engl. J. Med. 2001;345(26):1863-1869
2. Klemm T, Duda S, Machann J, et al. MR imaging in the presence of vascular stents: A systematic assessment of artifacts for various stent orientations, sequence types, and field strengths. J. Magn. Reson. Imaging 2000;12(4):606-615
3. von zur Mühlen C, Reiss S, Krafft AJ, Besch L, Menza M, Zehende M, et al. Coronary magnetic resonance imaging after routine implantation of bioresorbable vascular scaffolds allows non-invasive evaluation of vascular patency. PLoS ONE (2018) 13(1): e0191413.
4. C.M. Campos, T. Muramatsu, J. Iqbal, et al. Bioresorbable drug-eluting magnesium-alloy scaffold for treatment of coronary artery disease. Int. J. Mol. Sci. 14 (12) (2013) 24492–24500
5. Garcia-Garcia HM, Haude M, Kayode Kuku, et al. In vivo serial invasive imaging of the second-generation drug-eluting absorbable metal scaffold (Magmaris — DREAMS 2G) in de novo coronary lesions: Insights from the BIOSOLVE-II First-In-Man Trial. Int. J. Cardiol. 255 (2018) 22-28
6. Wehrli FW. Magnetic
resonance of calcified tissues. J Magn Reson. 2013 April ; 229: 35–48
Figures