2068
Free-breathing renal MR angiography using NATIVE TrueFISP: A comparison of different triggering techniques1Siemens Shenzhen Magnetic Resonance Ltd., ShenZhen, China
Synopsis
Non-contrast renal magnetic resonance angiography (MRA) is particularly valuable since contrast agents increase the risk of the Nephrogenic Systemic Fibrosis for the patients with renal failure. NATIVE TrueFISP together with triggering technique is commonly used for free breathing renal MRA. Here, we use 2D-PACE (Prospective Acquisition CorrEction) for respiratory triggering, therefore no external gating devices are needed and the preparation time is saved. The result shows that the image quality achieved by 2D PACE is comparable or superior to the conventional triggering techniques, which promises to be an alternative triggering method for renal MRA in clinical routine.
Purpose
Non-contrast MR angiography (MRA) is particularly valuable for renal arteries imaging, since contrast agents increase the risk of the nephrogenic systemic fibrosis for patients with renal failure [1]. NATIVE TrueFISP has been proved to be an effective way for non-contrast renal artery MRA [2-3]. To date, the two most widely used triggering techniques for free breathing imaging in clinical have been the respiratory belt (RESP) technique and the combined usage of ECG-triggering and navigator (ECG & NAV). In this abstract, we propose to integrate 2D-PACE (Prospective Acquisition CorrEction) technique [4] into NATIVE TrueFISP for respiratory triggering and compare it with the other conventional triggering techniques.Methods
8 healthy volunteers (mean age, 29±9 years; age range, 19-46 years) underwent renal MRA with IRB approval. All the measurements were performed on a 1.5T MR system (MAGNETOM Aera, Siemens Healthineers, Germany) with Body18 and spine array coils. The imaging parameters for the NATIVE TrueFISP sequence were TE = 1.52ms, flip angle = 90°, BW = 783Hz/Pixel, FOV = 340×243mm2, resolution = 1.1×1.1×1.1mm3, slices per slab = 72, in-plane GRAPPA factor = 2. For the ECG & NAV approach, shots per slice = 2, TI depends on R-R interval, accept window = ±3mm. For RESP technique, shots per slice = 1, TI = 1100ms, threshold = 40%. The parameters for the NATIVE TrueFISP triggered by 2D PACE are identical to ones used in the RESP technique. In addition, phase scout mode was used and the navigator with coronal orientation was manually positioned in liver. Accept window = ±30%, accept positon = 20%, which can make the triggering point ahead and ensure the data acquired in the expiration duration (Fig.1). The MIP images for renal arteries were reviewed by two independent observers. The left and right renal arteries are scored separately according to the following 5-point scale: 1, unacceptable (invisible ostia of renal arteries); 2, poor (ostia and proximal main renal arteries visible); 3, fair (distal main renal arteries and primary branches visible); 4, good (secondary branches visible); 5, excellent (tertiary branches visible).Results
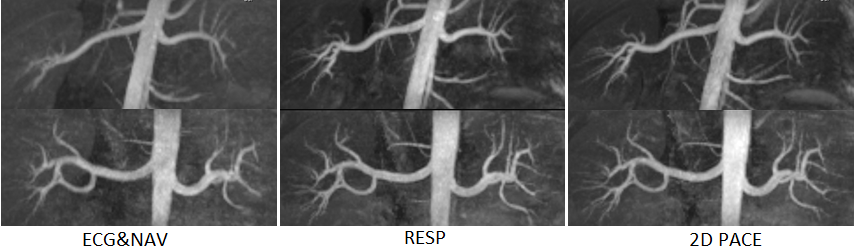
The average scores and total scan time of NATIVE TrueFISP using the three different triggering techniques are shown in table 1. Note that the mean scan time is similar for all triggering methods. For overall image quality, the 2D PACE and RESP were similar and both superior to the ECG& NAV. The MIP images show that the depiction of the tertiary branches of renal arteries was insufficient in some instances with ECG & NAV method (Fig.2).Discussion
The preparations for three triggering methods are quite different. The preparation steps for NAV & ECG method are as follows: 1, place ECG electrodes on the volunteer chest; 2, position the navigator on the dome of the diaphragm; 3, page through the axial slices to ensure the navigator does not overlap the renal arteries. Therefore it is time consuming and operator depended. For the RESP technique, the operator needs to place the respiratory belt around the upper abdomen of the volunteer to get the triggering signal. It is easy to operate and time saving in comparison to the ECG&NAV. For 2D PACE method, the operator only needs to check whether the 2D PACE navigator is in liver before the scanning. It is the most convenient one among three triggering methods. In addition, there is no external gating device needed in the proposed method, which helps make the patients more comfortable.Conclusion
The study has shown that the image quality of NATIVE TrueFISP using 2D PACE is comparable to that using RESP and much outperformed than that using the ECG & NAV. Moreover, it is easy to use, patient friendly and time efficient, holding a great promise as an alternative triggering method for renal artery MRA in clinical routine. Future work will focus on the improvement and clinical evaluation on patients.Acknowledgements
The author thanks Muhammed Labeeb and Shaorui Li for scoring the images, Dr. Wei Liu for reviewing the abstract.References
1. Grobner T, Prischl FC. Gadolinium and nephrogenic systemic fibrosis. Kidney Int. 2007;72(3):260-264.
2. Gandy S J, P. Guntur Ramkumar, Waugh S A et al. Non-contrast Enhanced Renal MR Angiography using NATIVE TrueFISP – Initial Experience for Clinical Imaging of Patients with Renovascular Disease. ISMRM 17 (2009), #404.
3 Saouaf R, Weiss S, Chithriki M, et al. Non-Contrast Renal MR Angiography at 3T Using NATIVE TrueFISP. The Internet Journal of Radiology. 2015;19(1) .
4 Morita S, Ueno E, Suzuki K, et al. Navigator-Triggered Prospective Acquisition Correction (PACE) Technique vs. Conventional Respiratory-Triggered Technique for Free Breathing 3D MRCP: An Initial Prospective Comparative Study Using Healthy Volunteers. JMRI. 2008; 28:673–677.
Figures
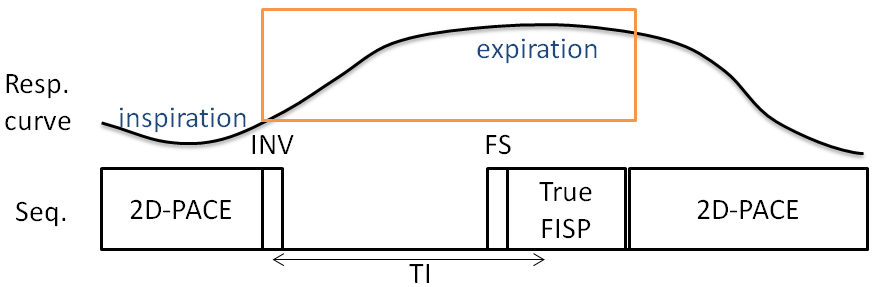
Fig.1: Diagram shows synchronization of image acquisition to respiratory cycle.
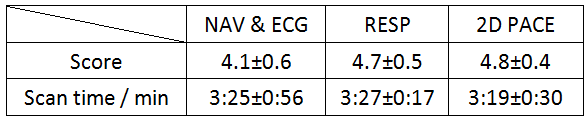
Table 1: average scores and scan time