2067
Highly Accelerated NCE-MRA Using Complex Subtraction with Intensity Correction: Improved Reconstruction Accuracy and Background Tissue Suppression1Department of Radiology, University of Cambridge, Cambridge, United Kingdom, 2Department of Radiology, Addenbrooke’s Hospital, Cambridge, United Kingdom
Synopsis
We propose a compressed sensing reconstruction method for highly accelerated subtractive non-contrast-enhanced MRA, based on complex subtraction in k-space. This method applies intensity difference correction between bright- and dark-blood image sets before reconstruction and uses a phase correction procedure to remove background artefacts caused by complex subtraction. Experimental results demonstrate improved background tissue suppression. Compared with magnitude subtraction approaches, the proposed method achieved higher reconstruction accuracy at large acceleration factors, permitting the use of higher acceleration factors without unacceptable loss of image quality.
Introduction
Subtractive Non-Contrast-Enhanced MR Angiography (NCE-MRA) methods display vasculature by subtracting dark-blood images (DBIs) from bright-blood images (BBIs). However, some static tissues have different intensity levels in BBIs and DBIs resulting in residual signal in the subtracted images. Our previous study proposed an optimised subtraction approach1, which corrects the intensity difference of background tissues before performing magnitude subtraction between the BBIs and DBIs.
Complex subtraction of k-space data (prior to reconstruction) can exploit the sparsity of the difference images for under-sampled datasets accelerated by compressed sensing (CS) or parallel imaging2,3. Applying the intensity correction prior to reconstruction could not only suppress the background tissue, but also potentially further increase the data sparsity and thus improve reconstruction accuracy at high acceleration factors (AF). However, weighted complex subtraction would also increase the negative signal after subtraction, which in magnitude images would appear as background artefacts due to the loss of polarity. Moreover, the weighting factor cannot be obtained directly from complex datasets.
This study proposes a reconstruction approach for complex subtraction with intensity correction. The weighting factors are calculated from the DBIs and BBIs generated by a quick CS reconstruction. Moreover, a phase correction procedure is applied to restore the polarity of the reconstructed data and null the negative background artefacts.
Method
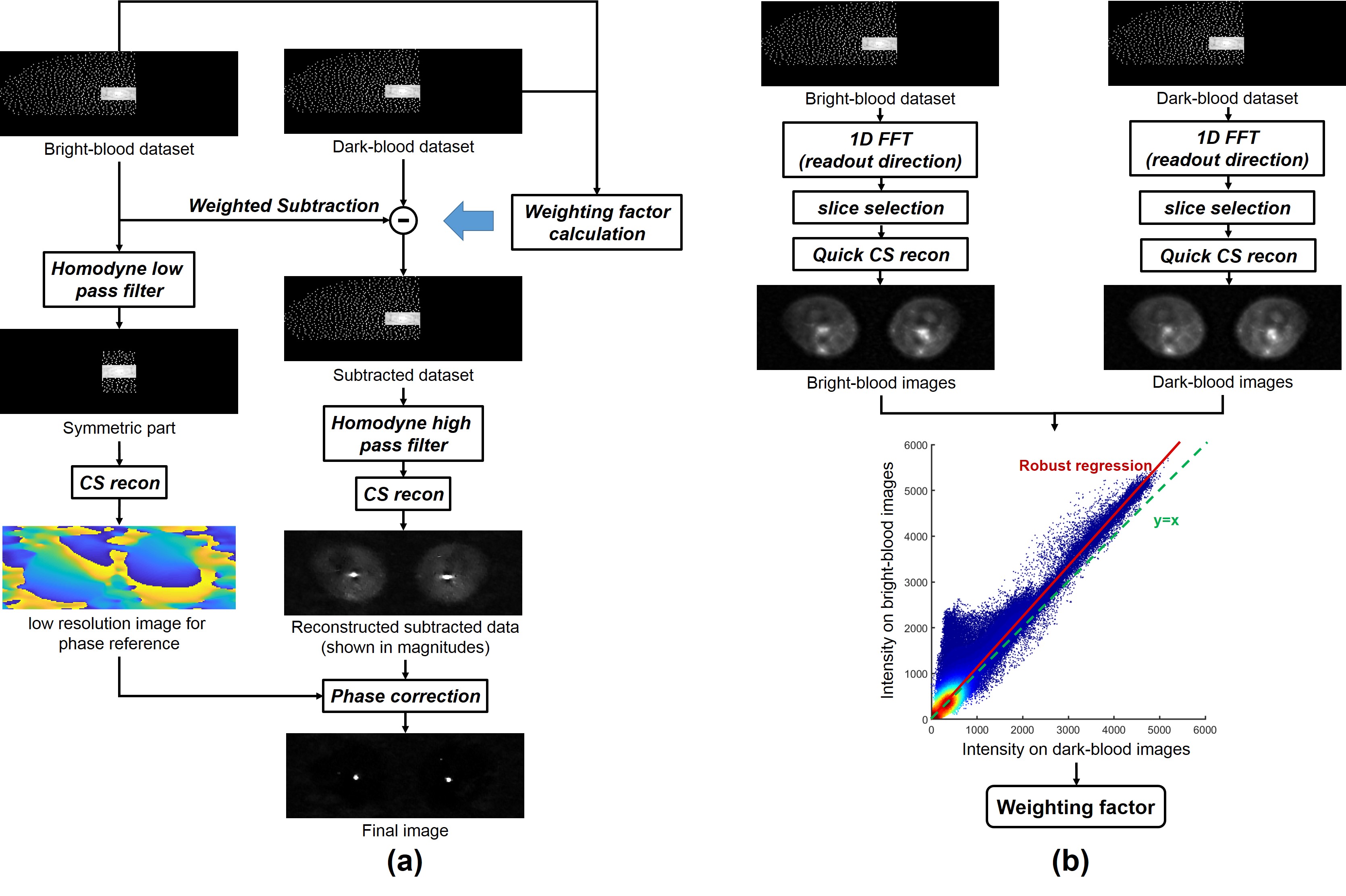
Fig. 1 shows the image reconstruction process and the weighting factor calculation procedure. Firstly, a quick CS reconstruction with only one iteration is performed on 10% equally-spaced slices selected along the readout direction. Secondly, a robust regression model using iteratively reweighted least squares4 is used to acquire the linear regression coefficient for the BBIs vs DBIs (weighted towards background pixels). Next, complex subtraction using the linear regression coefficient as the weighting factor is performed on the k-space data. A CS reconstruction with 12 iterations is then performed on the full subtracted dataset. Finally, a background phase reference is reconstructed from the symmetric central part of the bright-blood dataset and is used to restore the polarity of the negative signal.
CS reconstruction is performed using the Split-Bregman algorithm5 with the finite-differences transform as the sparsifying transform. The Split-Bregman algorithm has a rapid convergence, allowing a CS reconstruction in only one iteration for the quick CS reconstruction procedure. SPIRiT6, in combination with CS reconstruction, was used for autocalibrating parallel imaging reconstruction.
Fully sampled femoral ECG-gated 3D fast spin-echo7 datasets (TR 3xRR interval, TE 60ms, ETL 90, matrix 224×224×80, slice thickness 2 mm, FOV 40 cm, acquisition time 15-20 minutes) were acquired from 5 healthy volunteers using a 1.5 T MRI system (GE Healthcare, Waukesha, WI). Under-sampling with an overall AF from 4 to 20 was performed on fully sampled data by using a Poisson-disk sampling pattern combined with partial Fourier in both ky and kz dimensions.
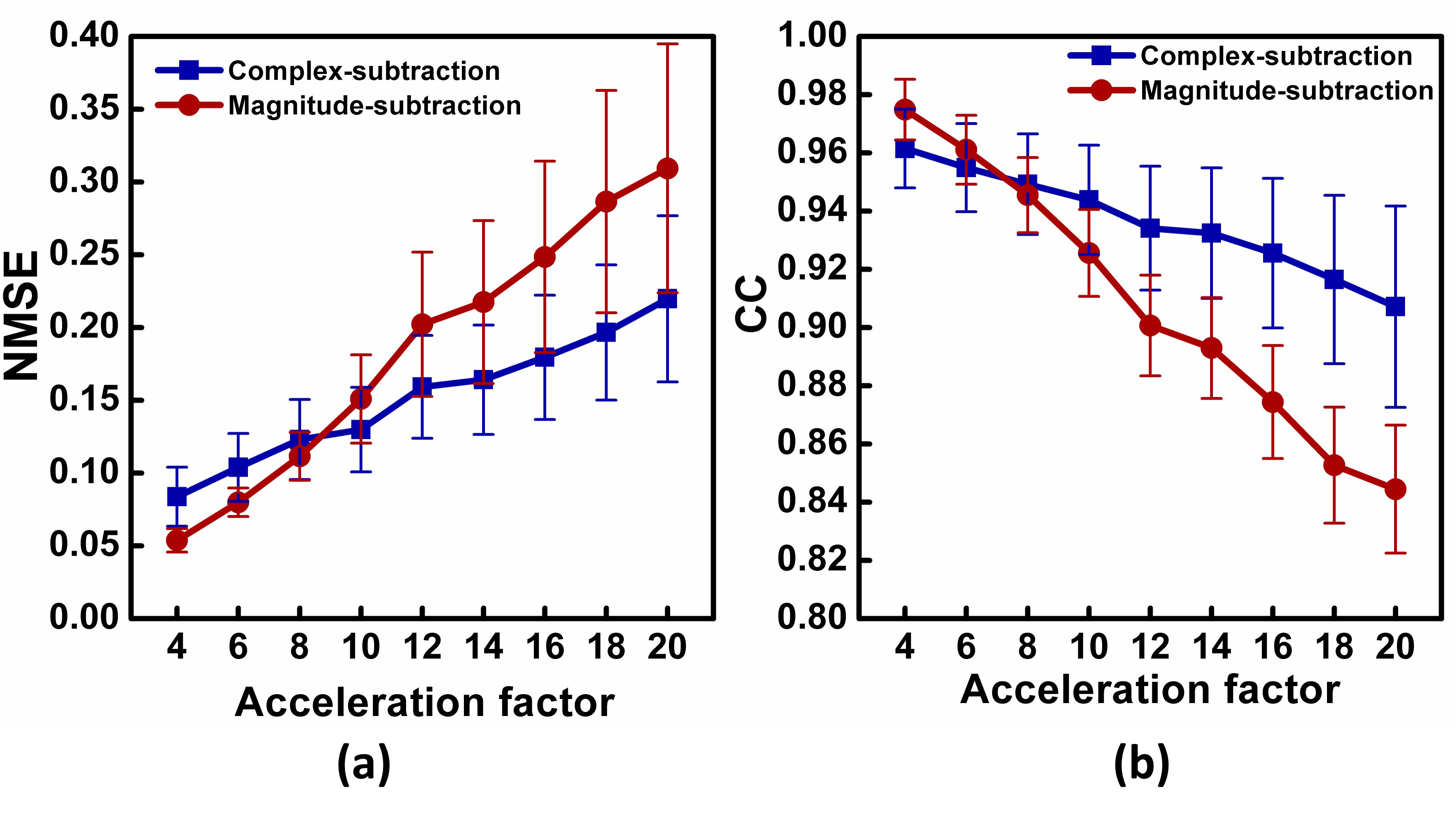
The fully sampled images were used as the reference. Phase correction was also performed on the fully sampled datasets when the intensity correction was applied. Reconstruction accuracy was assessed using correlation coefficients (CC) and the normalized mean square error (NMSE) calculated between the reference images and the reconstructed images with different AF.
Results and discussion
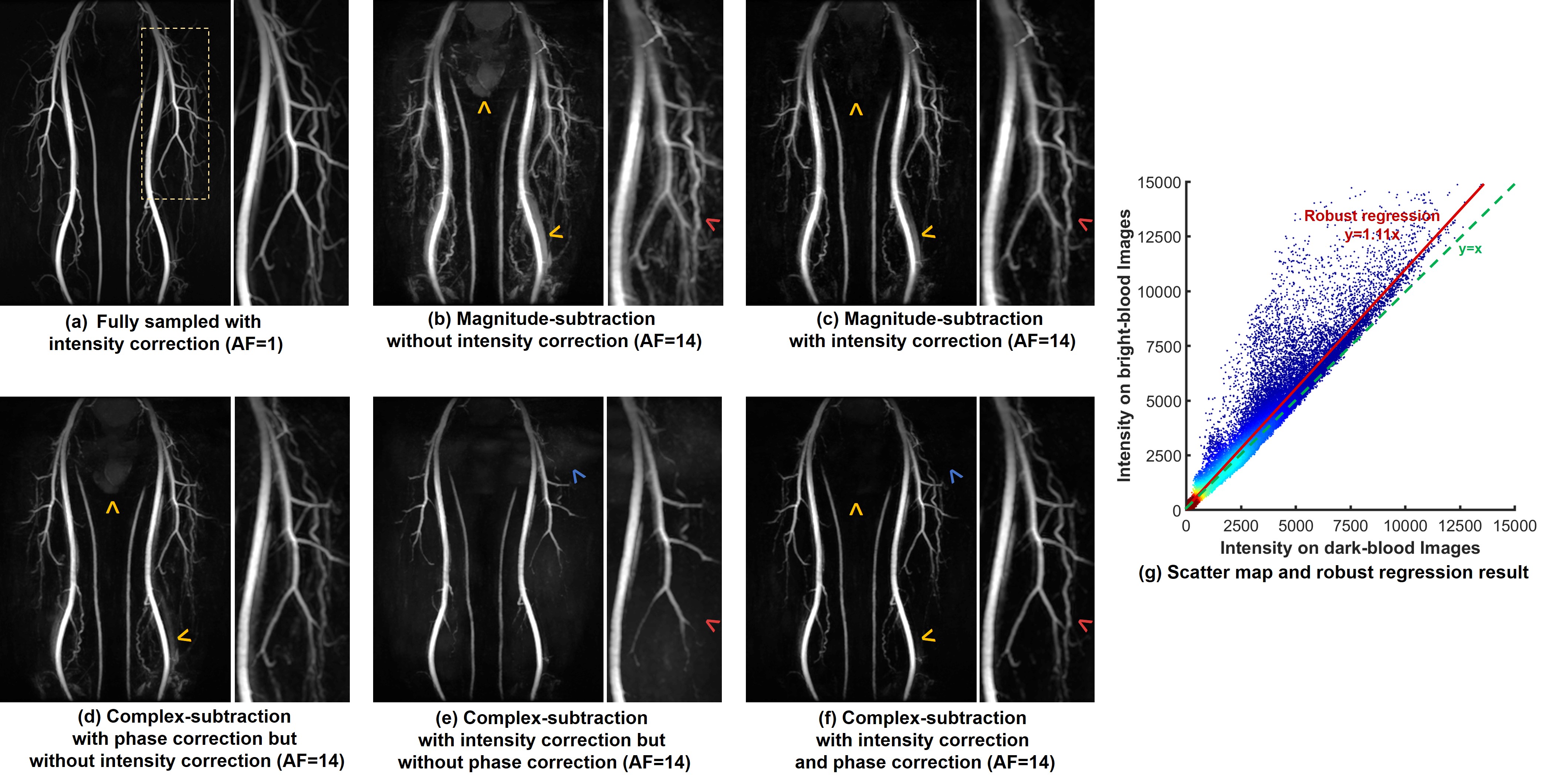
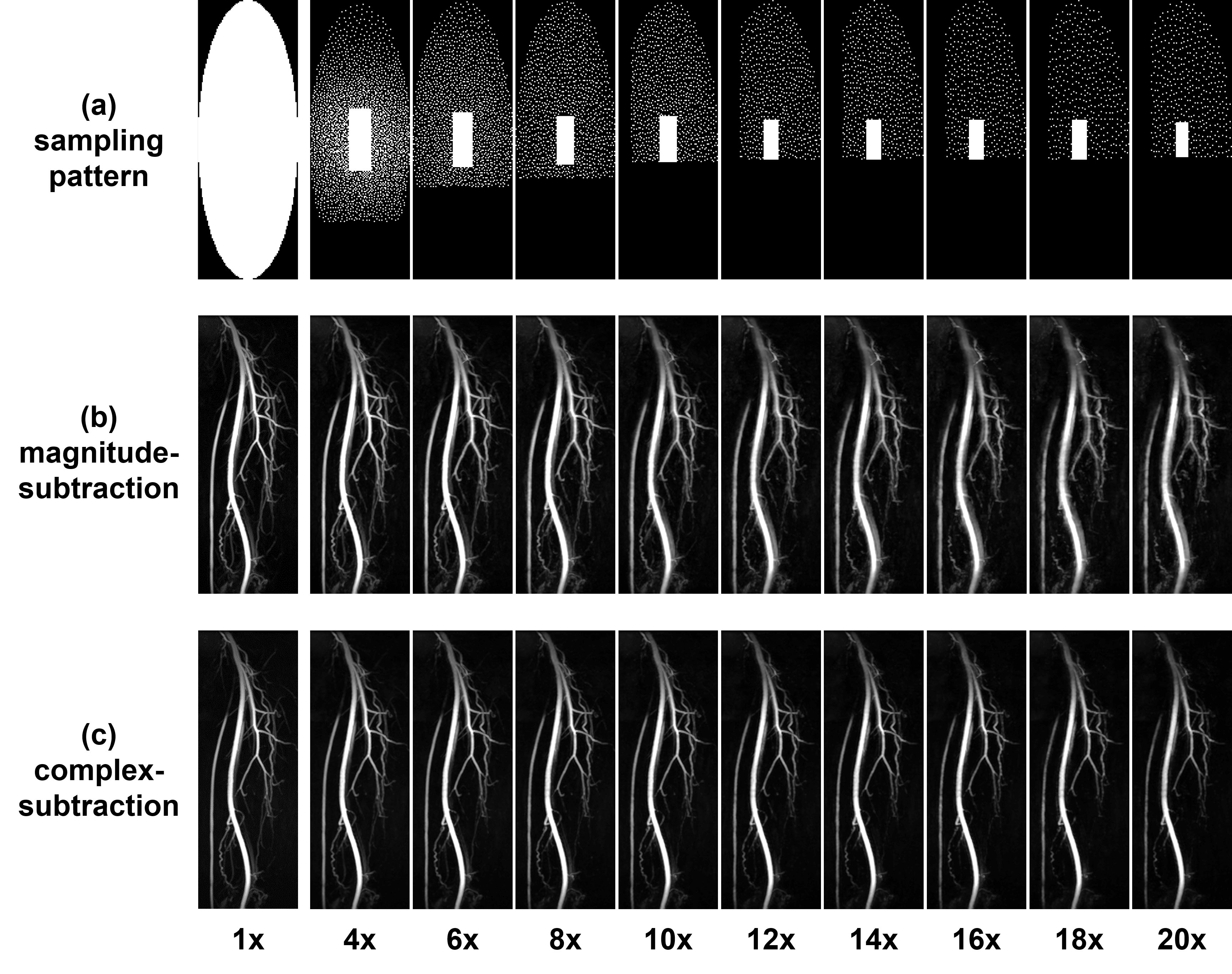
Fig. 2 compares different reconstruction methods for a dataset sampled with an AF of 14. It can be observed that the introduction of intensity correction improved the suppression of background tissue (yellow arrows) in both magnitude subtraction and complex subtraction, while the visualisation of arteries was not affected. However, the suppression is more thorough in complex subtraction (f). The complex subtraction achieved better image quality compared with magnitude subtraction, especially in the depiction of small arteries (red arrows). Background artefacts can be observed in complex subtraction without phase-correction (blue arrow), which could mask small arteries (red arrows). Fig. 3 shows the performance of complex subtraction and magnitude subtraction with intensity correction under the AF from 4 to 20. The average NMSE and CC over 5volunteers are shown in Fig. 4. Both magnitude subtraction and complex subtraction had good performance for small acceleration factors. However, complex subtraction demonstrates lower NMSE and higher CC when AF is larger than 8. Increased artefacts and residual venous signal can be observed on magnitude subtraction results at large AF, whereas complex subtraction results show clear arterial depiction and low noise level even with the AF of 20 in this case.Conclusion
The proposed CS reconstruction with complex subtraction and intensity correction improved background tissue suppression and reconstruction accuracy. Compared with magnitude subtraction approaches, the proposed CS reconstruction permits the use of larger acceleration factors without unacceptable loss of image quality.
Acknowledgements
The authors acknowledge the support of the Addenbrooke’s Charitable Trust and the NIHR Cambridge Biomedical Research Centre. Hao Li acknowledges the China Scholarship Council and Cambridge Trust for fellowship support. The authors thank Joshua Kaggie for providing the high-performance computer.
References
1. Li H, Wang S, Priest AN, Graves, MJ, Lomas DJ. An optimised subtraction approach for subtractive NCE-MRA techniques based on principal component analysis, ISMRM. 2018: 922.
2. Storey P, Otazo R, Lim RP, Kim S, Fleysher L, Oesingmann N, Lee VS, Sodickson DK. Exploiting sparsity to accelerate noncontrast MR angiography in the context of parallel imaging. Magn Reson Med. 2012;67(5):1391-1400.
3. Koktzoglou I, Sheehan JJ, Dunkle EE, Breuer FA, Edelman RR. Highly accelerated contrast-enhanced MR angiography: Improved reconstruction accuracy and reduced noise amplification with complex subtraction. Magn Reson Med. 2010;64(6).
4. Holland PW, Welsch RE. Robust regression using iteratively reweighted least-squares. Communications in Statistics - Theory and Methods, 6:9, 813-827.
5. Goldstein T, Osher S. The split Bregman method for L1-regularized problems. SIAM J Imaging Sci. 2009;2:323.
6. Lustig M, Pauly JM. SPIRiT: Iterative self-consistent parallel imaging reconstruction from arbitrary k-space. Magn Reson Med. 2010;64(2):457-471.
7. Miyazaki M, Sugiura S, Tateishi F, Wada H, Kassai Y, Abe H: Non-contrast-enhanced MR angiography using 3D ECG-synchronized half-Fourier fast spin echo. J Magn Reson Imaging 2000; 12:776–783.
Figures