2064
Non-Contrast-Enhanced zTE MR Angiography of Intracranial Atherosclerotic Disease1GE Healthcare, MR Research, Beijing, China, 2Department of Radiology, Affiliated Hospital of Xuzhou Medical University, Xu Zhou, China, 3GE Healthcare, MR Enhanced Application, Beijing, China
Synopsis
To investigate if zero-echo-time magnetic resonance angiography (zTE-MRA) is feasible in the characterization of intracranial atherosclerotic disease, we measured in this study a large population with atherosclerotic disease confirmed clinically. The acquired zTE-MRA images were thus compared systematically with those using time-of-flight (TOF)-MRA technique. Serving digital subtraction angiography (DSA) as a reference, zTE-MRA showed comparable imaging quality with DSA in the aspect of flow signal in the parent artery and higher signal intensity with less artifact than TOF-MRA. We therefore demonstrated that zTE-MRA could be a promising technique and further applied in the clinic routinely for patients with atherosclerotic disease.
Introduction
Cerebral vascular disease, as a crucial factor of hemorrhage and ischemia, has been usually diagnosed using digital subtraction angiography (DSA) but with risks of radiation and invasion. Magnetic resonance angiography (MRA), as a radiation free imaging technique, can be applied as a promising alternative for vascular evaluation1. In particular, a so called zero echo time (zTE) radial arterial spin labeling (ASL) MRA technique, inheriting a continuous ASL strategy and a zTE radial acquisition read-out, has shown its potential in the assessment of intracranial aneurysm and stent2,3.
However, it is still unknown if this novel MRA approach is also feasible in the diagnosis of atherosclerotic disease. To investigate this, in this study we applied this zTE-MRA technique in a large clinical population with atherosclerotic disease confirmed. Time-of-flight (TOF)-MRA images was also acquired for comparison and DSA imaging was applied and served as a reference.
Materials and Methods
Subjects
80 patients (mean age: 70.5±12.4 years old), confirmed with atherosclerotic disease clinically, were recruited in this study for MRI experiments. Written informed consent was obtained from each of them. 19 patients of them were also measured with DSA.
MRI Experiments
All MRI experiments were performed on a 3T MR system (Discovery 750w, GE Healthcare, USA) along with a 24-channel head-neck joint coil.
For zTE-MRA measurement, the scan parameters included a field-of-view (FOV) of 200X200mm covering the region from the parietal to the mandible, matrix size=166x166, repetition time (TR)=862ms, echo time (TE)=16μs, number of slices=332 and slice thickness=0.6mm. The scan time was 6 minutes 51s.
A TOF-MRA sequence was also applied to cover mesencephalon to cingulate cortex area with a FOV of 220x220mm. Other scan parameters were of matrix size=512x192, TR=20ms, TE=3.4ms, number of slices=172 and slice thickness=0.5mm. The acquisition time was 4 minutes 41s.
Data analysis
All acquired zTE- and TOF-MRA images were reconstructed with the maximum intensity projection and volume rendering methods, respectively, at a GE MR workstation (AW 4.6, GE Medical Systems, USA).
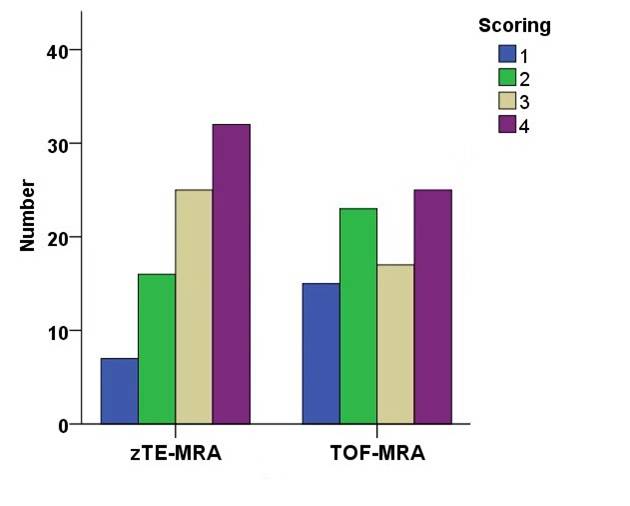
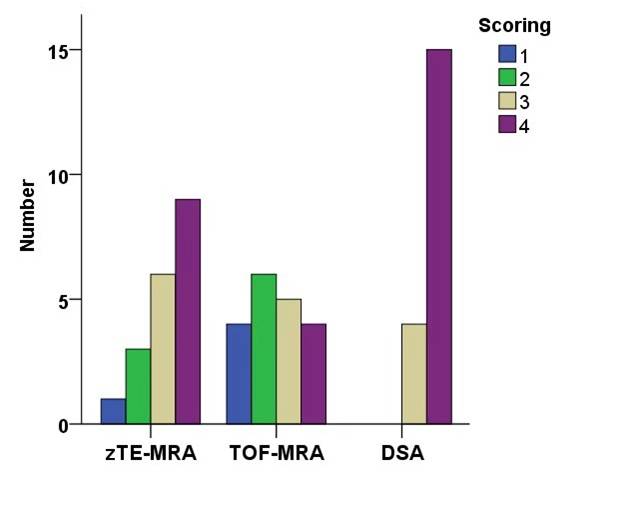
Two senior radiologists were employed to independently analyze the reconstructed images in the aspects of susceptibility artifact intensity and flow signal in the parent artery. A 4-point scale (4=no susceptibility signal loss, 3=minimal signal loss, 2=moderate signal loss, compromising image assessment, and 1=severe signal loss, preventing image evaluation) was applied to rate susceptibility artifact intensity for images. To score the flow signal in the parent artery, DSA imaging was served as a reference and a different 4-point rule was used, i.e., 4=excellent quality, equal to DSA images, 3=good quality with minimal blurring or artifacts, 2=poor quality with structures slightly visible and significant blurring, and 1=not visible.
The statistical analyses were performed using SPSS software 18.0 (IBM, Chicago, IL). Weighted kappa (κ) statistics was used to assess inter-observer agreement. The embedded Wilcoxon rank test toolbox was used to evaluate the difference of image quality in the aspects of susceptibility artifact intensity and flow signal in the parent artery between zTE- and TOF-MRA images, respectively. The significant threshold was set as p=0.05. In addition, Spearman’s correlation analysis was also applied to separately estimate the correlation between zTE-MRA and DSA and between TOF-MRA and DSA.
Results
A high inter-observer agreement was confirmed for evaluating zTE- and TOF-MRA images (weighted κ=0.78).
The images acquired by zTE-MRA showed significant higher quality than TOF-MRA images in the aspect of susceptibility artifact signal intensity (mean score: 3.02±0.97 vs 2.65±1.12; p=0.03; Figs.1,3,4).
As a reference for flow signal in the parent artery, the mean level of DSA images was 3.79±0.42 over 19 patients. In comparison, more comparable values were found in the zTE-MRA images (3.21±0.92) , which is significantly higher (p=0.029) than that in the TOF-MRA images (2.47±1.07; Figs.2-4).
In addition, both strong correlations were observed between zTE-MRA and DSA results (r=0.65, p=0.003), and between TOF-MRA and DSA results (r=0.50, p=0.03).
Discussion and Conclusion
In this study we investigated the feasibility of zTE-MRA in the diagnosis of atherosclerotic disease. After comparing with TOF-MRA results, more robust performance was observed in depicting cerebral vascular disease with higher signal intensity with less artifact, stronger flow signal in the artery and consistent findings with DSA served as a reference. In addition, due to the intrinsic properties, zTE-MRA is less sensitive to movement artifacts and can cover larger area with additional findings2.
In conclusion, due to the superior performance shown above, zTE-MRA technique can thus, be suggested as a routine method applied for patients with atherosclerotic disease in the clinic.
Acknowledgements
No acknowledgement found.References
1. Bash S, Villablanca JP, Jahan R, et al. Intracranial Vascular Stenosis and Occlusive Disease: Evaluation with CT Angiography, MR Angiography, and Digital Subtraction Angiography. AJNR Am J Neuroradiol. 2005;26 (5):1012-1021.
2. Shang S, Ye J, Luo X, et al. Follow-up assessment of coiled intracranial aneurysms using zTE MRA as compared with TOF MRA: a preliminary image quality study. Eur. Radiol. 2017:27(10):4271-4280.
3. Irie R, Suzuki M, Yamamoto M, et al. Assessing Blood Flow in an Intracranial Stent: A Feasibility Study of MR Angiography Using a Silent Scan after Stent-Assisted Coil Embolization for Anterior Circulation Aneurysms. AJNR Am J Neuroradiol. 2015;36 (5):967-970.
Figures