2063
Acceleration of whole-heart coronary MR angiography using 3D non-selective bSSFP with Compressed SENSE1Department of Radiological Services, Tokyo Women's Medical University, Tokyo, Japan, 2Department of Diagnostic Imaging and Nuclear Medicine, Tokyo Women's Medical University, Tokyo, Japan, 3Philips Electronics Japan, Tokyo, Japan
Synopsis
Whole heart coronary magnetic resonance angiography (WHC-MRA) has a limitation of long scan time, which often causes degradation of image quality. 3D non-selective balanced TFE (bTFE) with shortening TR can reduce the scan time. However, it is yet not applied for WHC-MRA. Compressed SENSE (C-SENSE) is suitable for subjects with a high sparse such as vessels and biliary trees, and can accelerate the scan time of WHC-MRA while ensuring the image quality. We propose a new combination of 3D non-selective bTFE with C-SENSE for WHC-MRA, and examine the image quality and the scan time in comparison to the conventional methods.
Introduction
Coronary magnetic resonance angiography (CMRA) is a promising noninvasive imaging modality for the detection of Coronary artery disease (1). CMRA mainly employs 3D balanced-SSFP (bSSFP) sequence and it has been used for coronary MRA at 1.5T because of its intrinsically high SNR and CNR (2). An important limitation of 3D bSSFP, however, is its relatively long imaging time (3) because CMRA basically needs cardiac synchronization and high resolution is required to visualize coronary artery with the vessel diameter less than 1 cm. 3D non-selective balanced TFE (3D nsbTFE) has the possibility to solve this problem. 3D nsbTFE enables shorter TR by not using the slice selective excitation (Fig. 1), resulting in increasing the TFE factor during one heartbeat. Therefore, we hypothesized that 3D nsbTFE can reduce scan time. In this study, we investigated the feasibility of 3D nsbTFE for CMRA by comparing with conventional bTFE sequence (conventional method). In addition, Compressed SENSE (C-SENSE) has recently been introduced as a new acceleration technique. We also combined C-SENSE to 3D nsbTFE and investigated to further accelerate the scan time of CMRA.Methods
[Subjects] WHC-MRA images with 6 healthy volunteers approved by the Institutional Review Board of our facility (6 males; age range: 30~44). [Materials] 1.5T MR system (Ingenia CX, Philips Healthcare) and dS Torso coil. We compared image quality and scan time among WHC-MRA using conventional method, 3D nsbTFE and 3D nsbTFE with C-SENSE. Three sequences were acquired with navigator and cardiac triggering using the following parameters; conventional method: FOV (mm) = 250×220, spatial resolution (mm) = 1.5×1.5×1.5, TR/TE (ms) = 3.5/1.77, flip angle (° ) = 70, SENSE factor = 2×1.3, slice orientation = transverse; 3D nsbTFE: FOV (mm) = 220×250, spatial resolution (mm) = 1.5×1.5×1.5, TR/TE (ms) = 2.3/1.19, flip angle (° ) = 70, SENSE factor = 2×1.3, slice orientation = coronal; 3D nsbTFE with C-SENSE: FOV (mm) = 220×250, spatial resolution (mm) = 1.5×1.5×1.5, TR/TE (ms) = 2.3/1.19, flip angle (° ) = 70, C-SENSE factor = 5, 7, 10, slice orientation = coronal. [Image analysis] Curved Planer Reconstructions (CPRs) were performed using Ziostation2 (Ziosoft Co, Tokyo) and image quality was evaluated by visual score at 10 places (RCA: #1, 2, 3, 4 LAD: #5, 6, 7, 8 CX: #11, 13) based on American Heart Association (AHA) classification. The visual evaluation items were three items of overall image quality, sharpness, noise and artifacts, we evaluated them as 4-point grades (grade “4” was excellent, “1” was severe) by two blinded readers (one radiologist and one radiological technologist).Results and Discussion
Figure 2 shows the representative images using conventional bTFE, nsbTFE and nsbTFE with several C-SENSE factors. In overall image quality, there was no significant difference between conventional method and 3D nsbTFE. For the image sharpness, 3D nsbTFE was lower than conventional method (P <0.05). Regarding the absence of noise and artifacts, 3D nsbTFE was significantly lower than conventional method (P <0.01). 3D nsbTFE reduced scan time by 34% compared with conventional method. In all visual evaluation subjects, there was no significant difference between 3D nsbTFE and 3D nsbTFE with C-SENSE factor 5 and 7; however, 3D nsbTFE with C-SENSE factor 10 was significantly lower than 3D nsbTFE (P <0.01). 3D nsbTFE with C-SENSE factor 7 sequence reduced scan time by 38% compared with 3D nsbTFE. Figure 3 shows the representative images using optimized nsbTFE protocol. The summary of visual evaluation and scan time is shown in Figure 4 and 5.Conclusion
WHC-MRA using 3D nsbTFE with C-SENSE can reduce scan time by 59% compared with conventional method while ensuring the image quality; it was suggested clinical utility.Acknowledgements
No acknowledgements found.References
(1) Teresa Correia et al. Technical note: Accelerated nonrigid motion‐compensated isotropic 3D coronary MR angiography. Med Phys. 2018 Jan; 45(1): 214–222. (2) Jingsi Xie et al. Whole-heart coronary magnetic resonance angiography at 3.0T using short-TR steady-state free precession, vastly undersampled isotropic projection reconstruction. J Magn Reson Imaging 2010 May;31(5):1230-5. (3) Mehdi H. Monghari et al. Three-dimensional Heart Locator and Compressed Sensing for Whole-heart Magnetic Resonance Angiography. Magn Reson Med. 2016 May; 75(5): 2086–2093. (4) Yuji Iyama, et al. Single-Breath-Hold Whole-heart Unenhanced Coronary MRA Using Multi-shot Gradient Echo EPI at 3T: Comparison with Free-breathing Turbo-field-echo Coronary MRA on Healthy Volunteers. Magn Reson Med Sci 2018 Apr 10; 17(2): 161–167.Figures
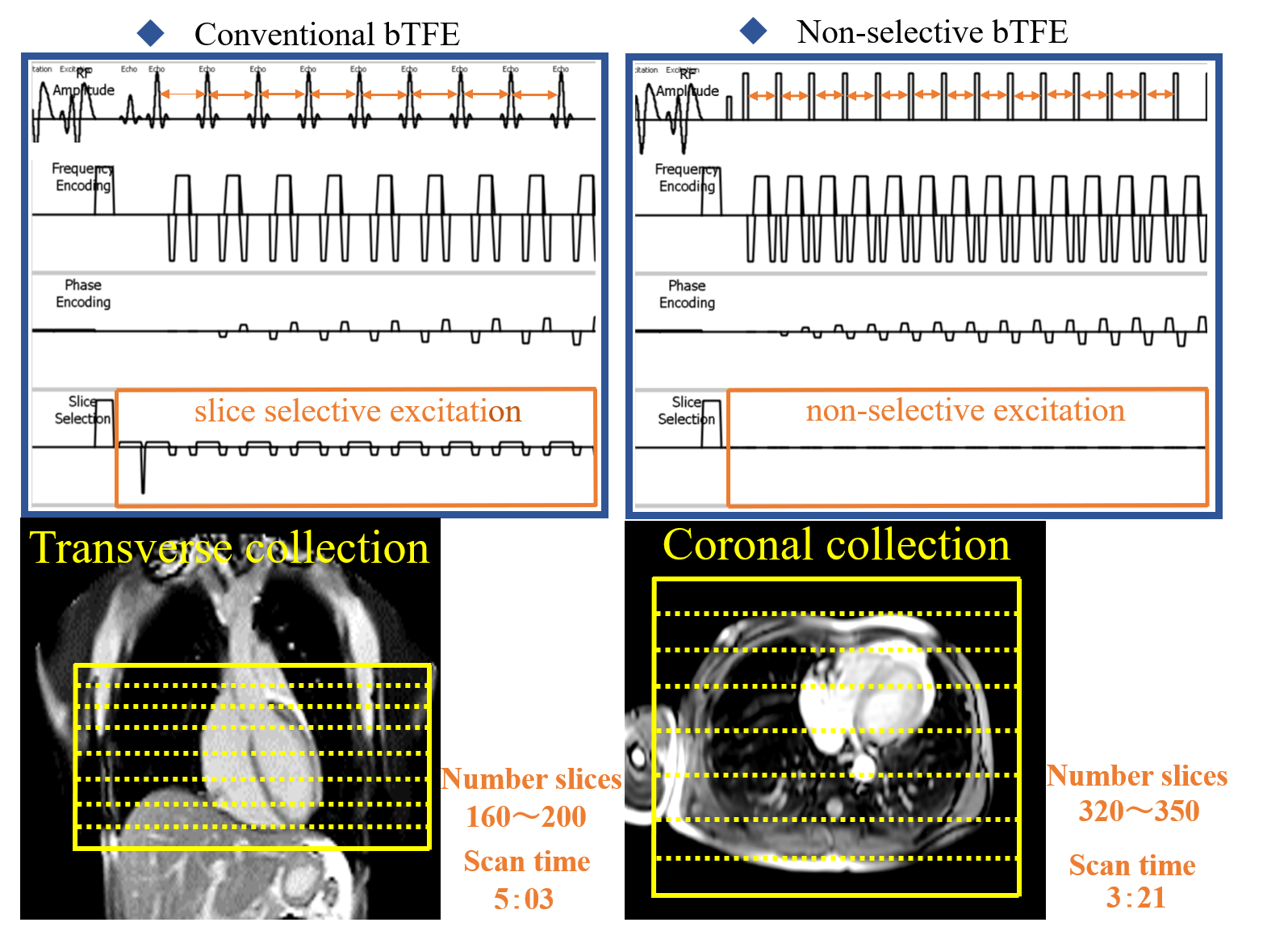
Figure 1
Sequence chart of conventional bTFE and non-selective bTFE and Slice orientation. Non-selective bTFE enables shorter TR by not using the slice selective excitation. Conventional bTFE sequence is transverse collection. In non-selective bTFE sequence, consider aliasing artifacts, coronal collection to include the body completely in the slice direction.
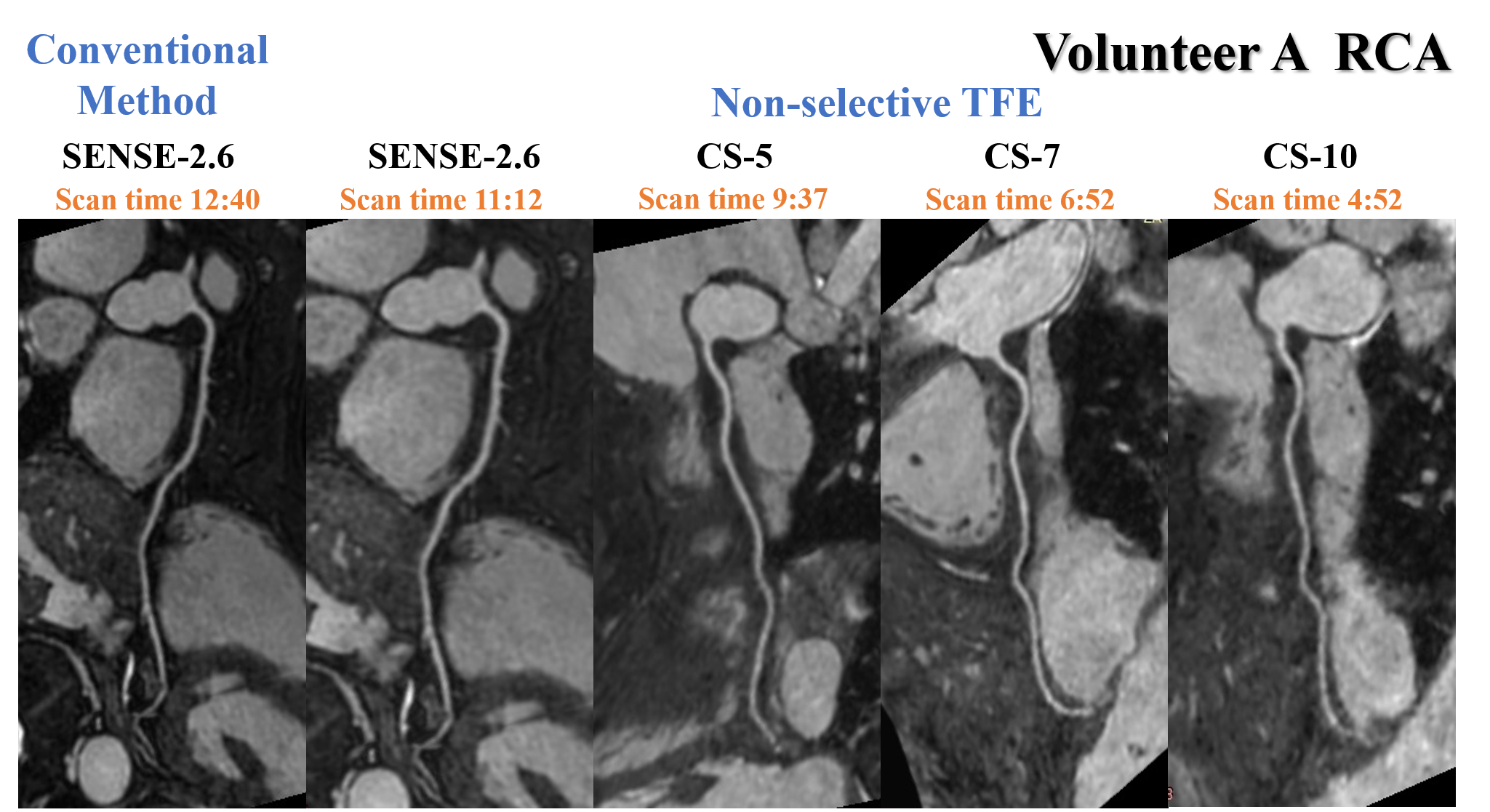
Figure 2
CPR images of RCA of volunteer A in conventional bTFE sequence and 3D non-selective bTFE sequence. 3D nsbTFE with C-SENSE 7 reduced scan time by 5 minutes and 48 seconds from conventional method while ensuring image quality.
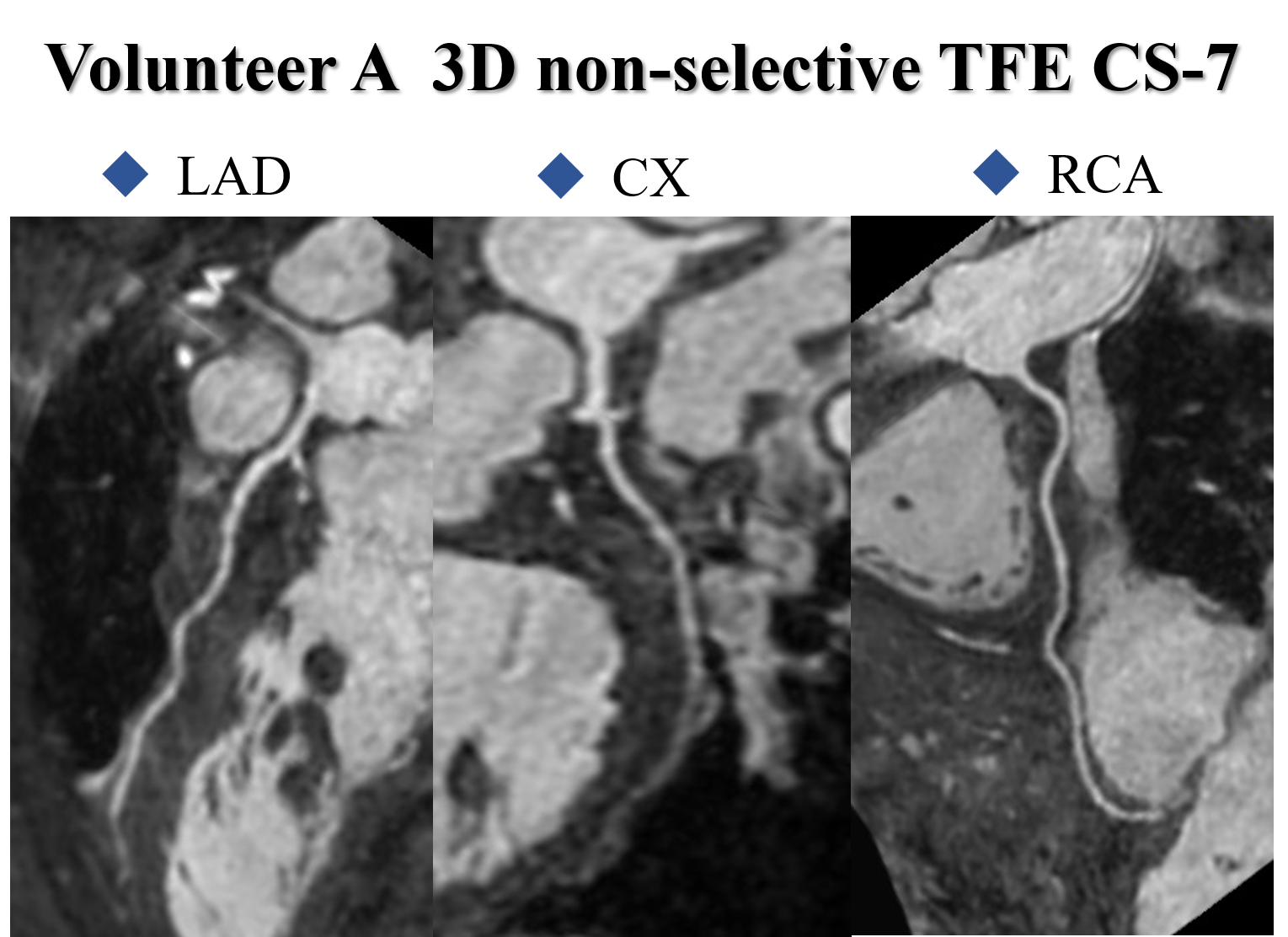
Figure 3
CPR images of coronary artery of volunteer A in 3D non-selective bTFE with C-SENSE factor 7 sequence. Scan time was 6:52 at collection efficiency of 40%.
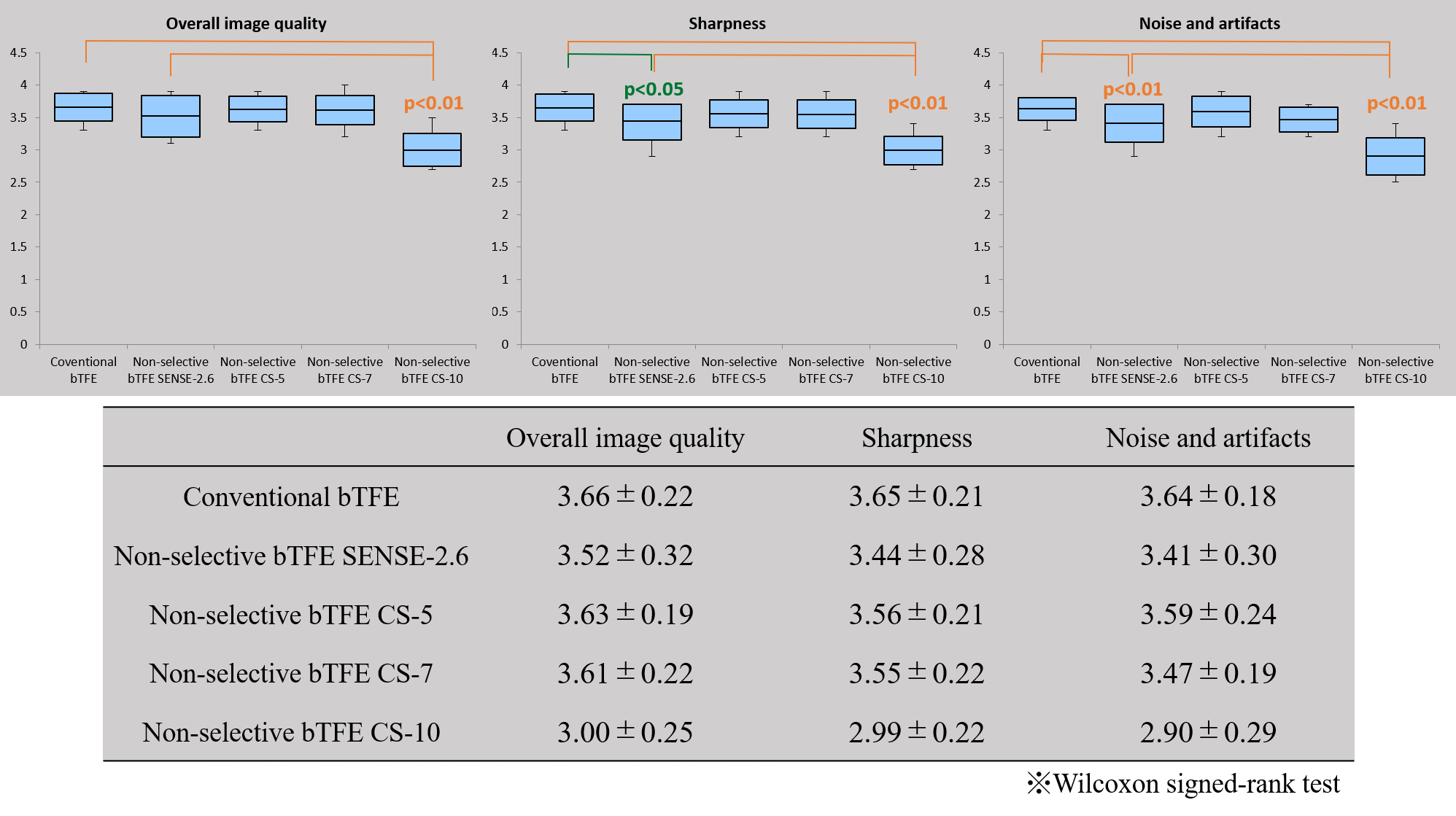
Figure 4
Result of visual evaluation. In overall image quality, there was no significant difference among conventional bTFE, 3D nsbTFE and 3D nsbTFE with C-SENSE factor 5 and 7; however, 3D nsbTFE with C-SENSE factor 10 was significantly lower than conventional bTFE (P <0.01). For the image sharpness, 3D nsbTFE was significantly lower than conventional bTFE (P <0.05); and 3D nsbTFE with C-SENSE factor 10 was significantly lower than conventional bTFE (P <0.01). Regarding the absence of noise and artifacts, 3D nsbTFE and 3D nsbTFE with C-SENSE factor 10 were significantly lower than conventional bTFE (P <0.01).
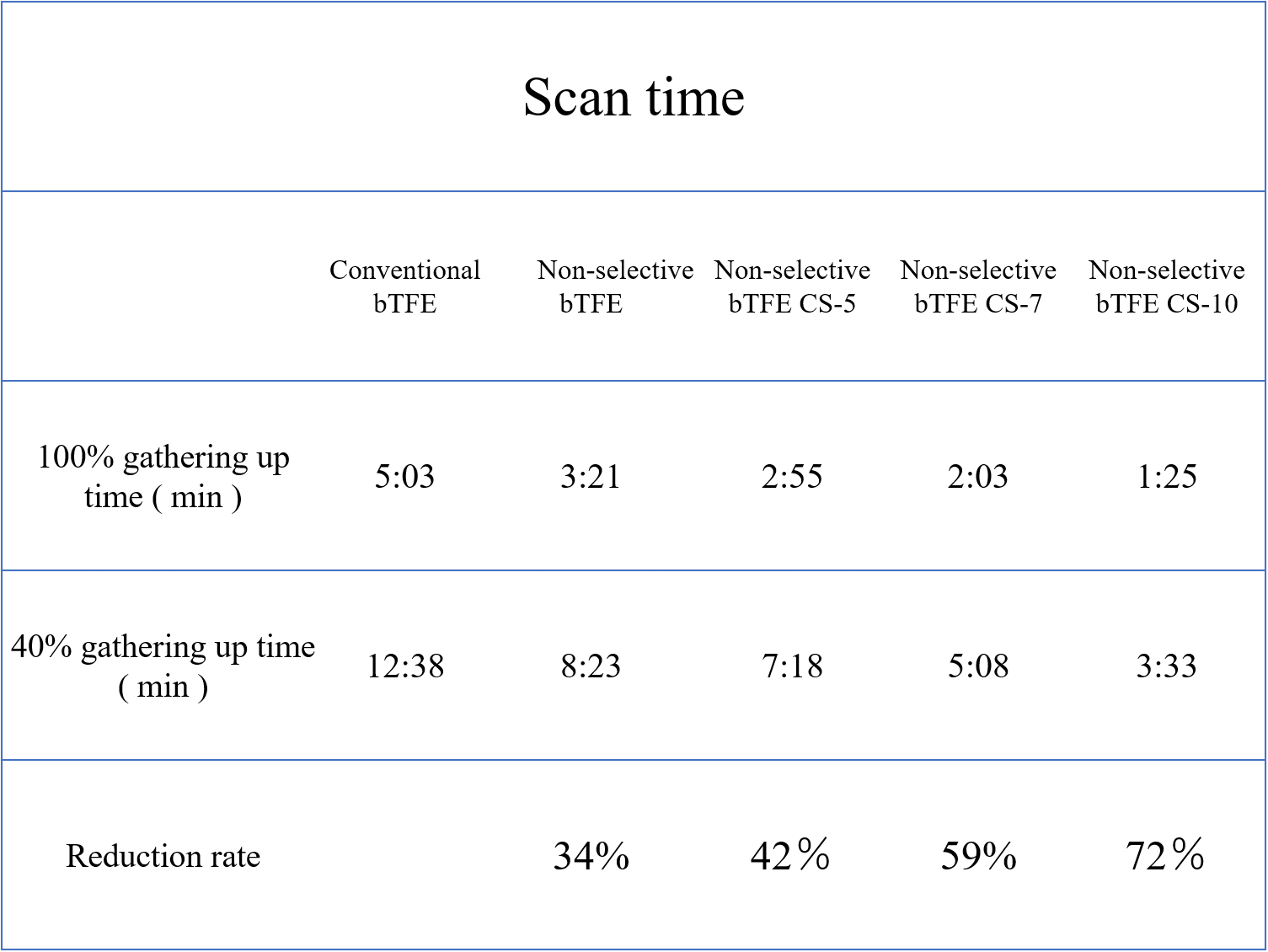
Figure 5
The average scan time of each sequence. The reduction rate is compared with the conventional bTFE. 3D non-selective bTFE with C-SENSE factor 7 sequence which had no significant difference in visual evaluation reduced scan time by 59% from conventional bTFE sequence.