2062
Non-Contrast-Enhanced Abdominal MRA at 3T using Velocity-Selective Pulse Trains1Department of Biomedical Engineering, Johns Hopkins Medical Institutions, Baltimore, MD, United States, 2Department of Radiology, Johns Hopkins University School of Medicine, Baltimroe, MD, United States, 3. F.M. Kirby Research Center for Functional Brain Imaging, Kennedy Krieger Institute, Baltimore, MD, United States, 4Department of Radiology, Xiangya Hospital, Central South University, Changsha, China, 5Division of Mechanical and Biomedical Engineering, Ewha Womans University, Seoul, Korea, Republic of, 6Department of Medicine, Case Western Reserve University, Cleveland, OH, United States
Synopsis
Non-contrast-enhanced (NCE) abdominal MR angiography (MRA) with large spatial coverage is clinically desired. The current method using spatially selective inversion (SSI) pulse to null static tissue and blood is only limited to small field of view (FOV) due to its sensitivity to slow arterial inflow. Velocity-selective inversion (VSI) based approach was shown to preserve the arterial blood inside the imaging volume at 1.5T. In this study, a novel strategy of VSI + VSS was proposed for abdominal MRA of large FOV, and its advantage over SSI based approach was demonstrated among healthy subjects at 3T.
INTRODUCTION
The main approach for non-contrast-enhanced (NCE) abdominal MR angiography (MRA) is to place a spatially selective inversion (SSI) pulse with a delay to null signal of static tissue and blood within the inversion slab and to allow inflow of upstream arterial blood1. Since a compromise has to be made between the exact background nulling time and sufficient arterial inflow time, this SSI based method is often limited to small field of view (FOV) and commonly applied for renal MRA2. A velocity-selective inversion (VSI) based approach was later developed for abdominal MRA to preserve the arterial blood inside the imaging volume at 1.5T3. Recently, a combination of SSI and velocity-selective saturation (VSS) was successfully demonstrated with superior background suppression for cerebral MRA at 3T4. In this study, we propose a novel strategy of VSI plus VSS for abdominal MRA of large FOV at 3T, and compare it with SSI plus VSS based approach.METHODS
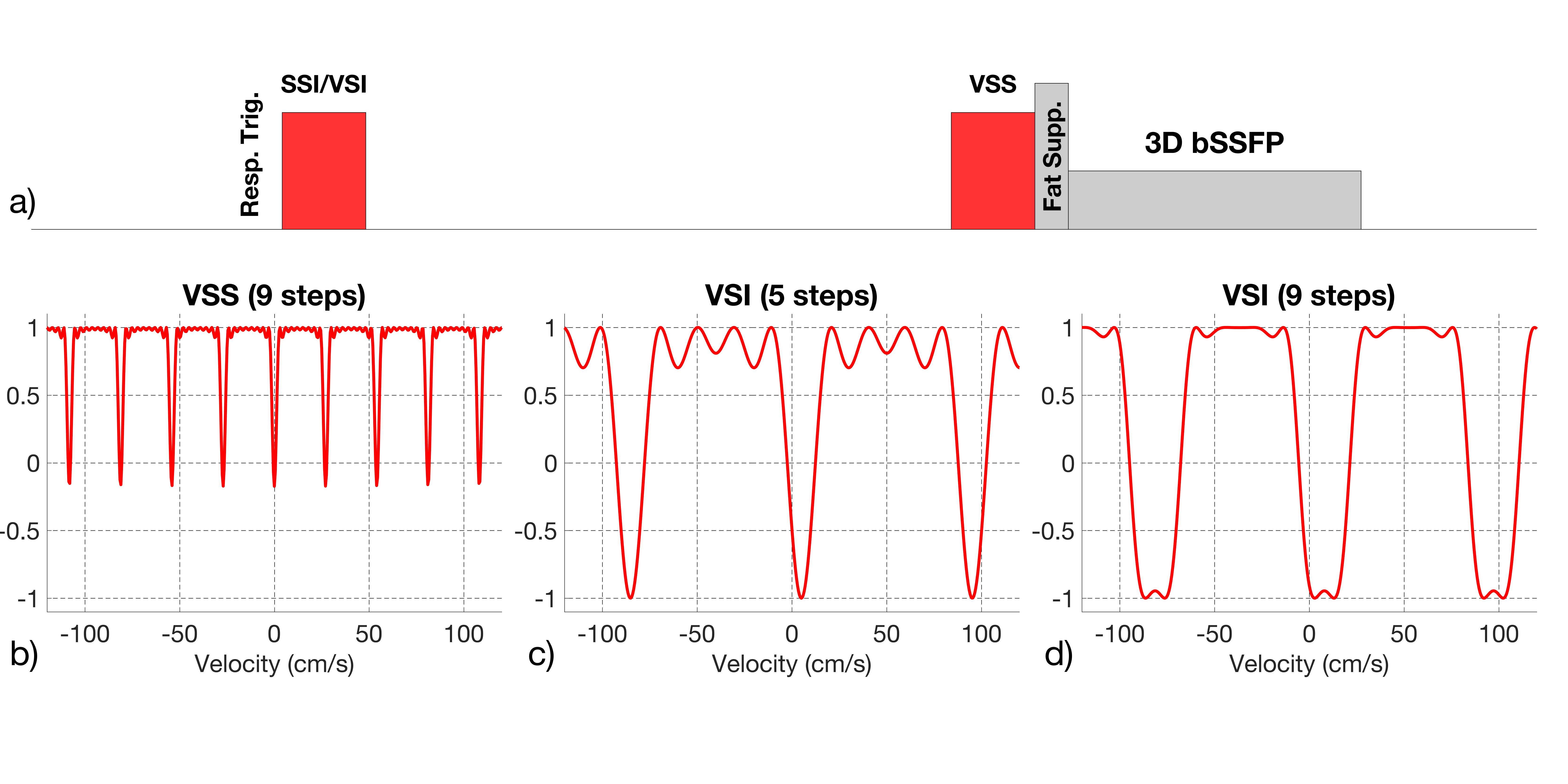
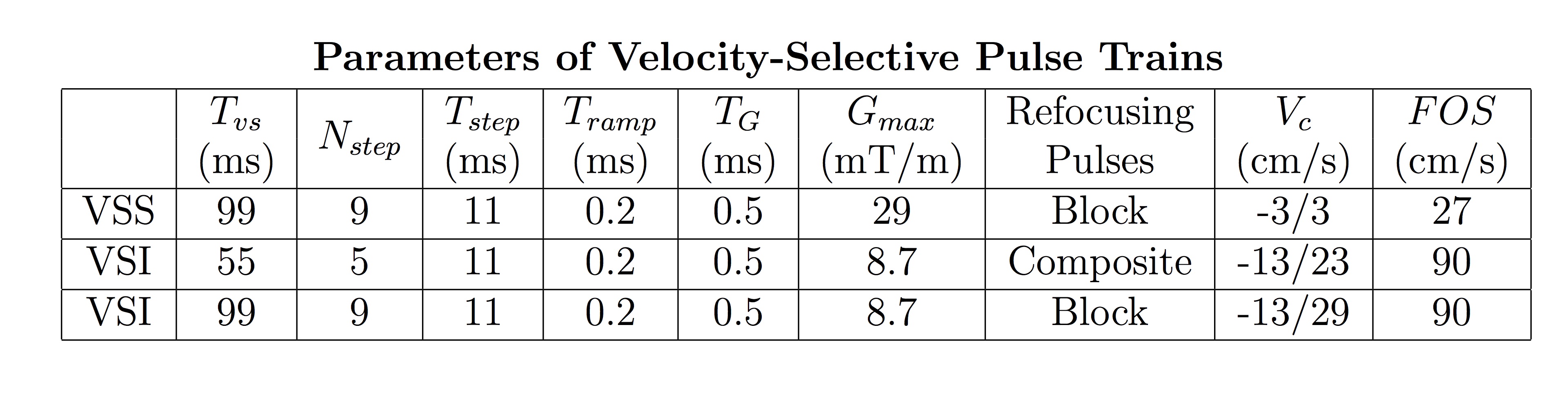
The pulse sequences used in this study are displayed in Fig. 1a. A VSS pulse train was placed right before acquisition modules to suppress static tissue. An adiabatic SSI pulse4 or a VSI pulse train was applied with inversion delays 1.2 sec and 0.9 sec, respectively, to null tissue background and venous signal. The SSI module was applied to a slab larger than the imaging volume by 10 cm in the foot direction to reduce inflow from femoral veins. When inversion pulses are not applied, the VSS module alone does not separate arterial and venous blood. Respirational triggering was utilized in this sequence. All VSS or VSI pulse trains were composed of a series of excitation pulses, interleaved with pairs of refocusing pulses and velocity-encoding gradient lobes4. VSS had 9 velocity-encoding steps with a 100° saturation band within ±3 cm/s (Fig. 1b). To null both small veins and the large upward inferior vena cava (IVC), 5-step and 9-step VSI were explored with 180° inversion band within [-13, 23] and [-13, 29] cm/s, respectively (Figs. 1c,d). Specific parameters for VSS and VSI pulse trains are shown in Table 1. All velocity-encoding gradients were applied to 45 degrees between foot head (FH) and left right (LR) directions.
Experiments
were performed on a 3T scanner
(Ingenia, Philips Healthcare) using a 32-channel chest coil for
reception. Comparisons of VSS,
SSI + VSS with 5-step and 9-step VSI + VSS protocols were conducted
respectively on 12 healthy subjects (24−63
years old,
6 females, 6 males).
Two subjects were scanned with both 5-step and 9-step VSI + VSS protocols. The acquisition parameters
for 3D bSSFP of a coronal slab are: FA = 110°, FOV =300(FH)
× 278(LR)
× 120(AP)mm3, resolution = 1.4
× 1.4
× 2mm3, TR/TE = 6.4/2.6ms,
BW =
1330.3Hz. Scan time was 2.2 min with a
compressed sensing (CS) factor of 8. Two-dimensional PC-MRA was acquired on several subjects in the abdominal aorta for velocity quantification.
RESULTS AND DISCUSSION
The comparison of VSS, SSI + VSS and 5-step VSI + VSS of 2 cases were displayed in Fig. 2. VSS greatly enhanced blood contrast and shows main abdominal vasculature, such as aorta, IVC, portal system, hepatic, renal and splenic vessels. Both SSI + VSS and VSI + VSS largely suppress veins and show arteries only: aorta, celiac trunk, common hepatic artery, splenic artery, superior mesentery artery, renal arteries and their branches. Fig. 3 shows the comparison of VSS, SSI + VSS and 9-step VSI + VSS of 2 cases. Detailed renal artery branches could be visible in SSI/VSI+VSS images.
For older participants, SSI + VSS scans were not able to show distal iliac arteries (Fig. 2), compared to the results of younger subjects (Fig. 3), due to their slower blood velocity (systolic peak velocity: ~ 60 cm/s vs. ~80 cm/s). SSI may lose proximal aorta signal (Figs. 2b, 3b) when heart apex is covered by the SSI slab. Inverted blood in heart apex flows into proximal abdominal aorta and shows low signal there.
When both the 5-step and 9-step VSI + VSS were applied, 5-step VSI + VSS yielded more detailed renal artery branches, while 9-step VSI + VSS provided better background suppression (Fig. 4).
CONCLUSION
A new 3D NCE abdominal MRA sequence for large spatial coverage was proposed that utilizes both advanced velocity-selective saturation and inversion pulse trains for background tissue suppression and artery-vein separation. Compared to SSI + VSS method, the advantage of VSI + VSS for its less sensitivity to slow arterial inflow is demonstrated among older healthy subjects.Acknowledgements
No acknowledgement found.References
1. Miyazaki M, Isoda H. Non-contrast-enhanced MR angiography of the abdomen. European journal of radiology 2011;80(1):9-23.
2. Parienty I, Rostoker G, Jouniaux F, Piotin M, Admiraal-Behloul F, Miyazaki M. Renal artery stenosis evaluation in chronic kidney disease patients: nonenhanced time-spatial labeling inversion-pulse three-dimensional MR angiography with regulated breathing versus DSA. Radiology 2011;259(2):592-601.
3. Shin T, Worters PW, Hu BS, Nishimura DG. Non-contrast-enhanced renal and abdominal MR angiography using velocity-selective inversion preparation. Magn Reson Med 2013;69(5):1268-1275.
4. Li W, Xu F, Schar M, Liu J, Shin T, Zhao Y, van Zijl PCM, Wasserman BA, Qiao Y, Qin Q. Whole-brain arteriography and venography: Using improved velocity-selective saturation pulse trains. Magn Reson Med 2018;79(4):2014–2023.
Figures