2061
The feasibility of high resolution vessel wall imaging (HR VWI) based minimum intensity projection (mIP) MRA for evaluating steno-occlusive MCA1Department of Radiology, Beijing Tiantan Hospitial, Capital Medical University, Beijing, China, 2Center for Biomedical Imaging Research, Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, China
Synopsis
Stenosis, distal branches
Introduction
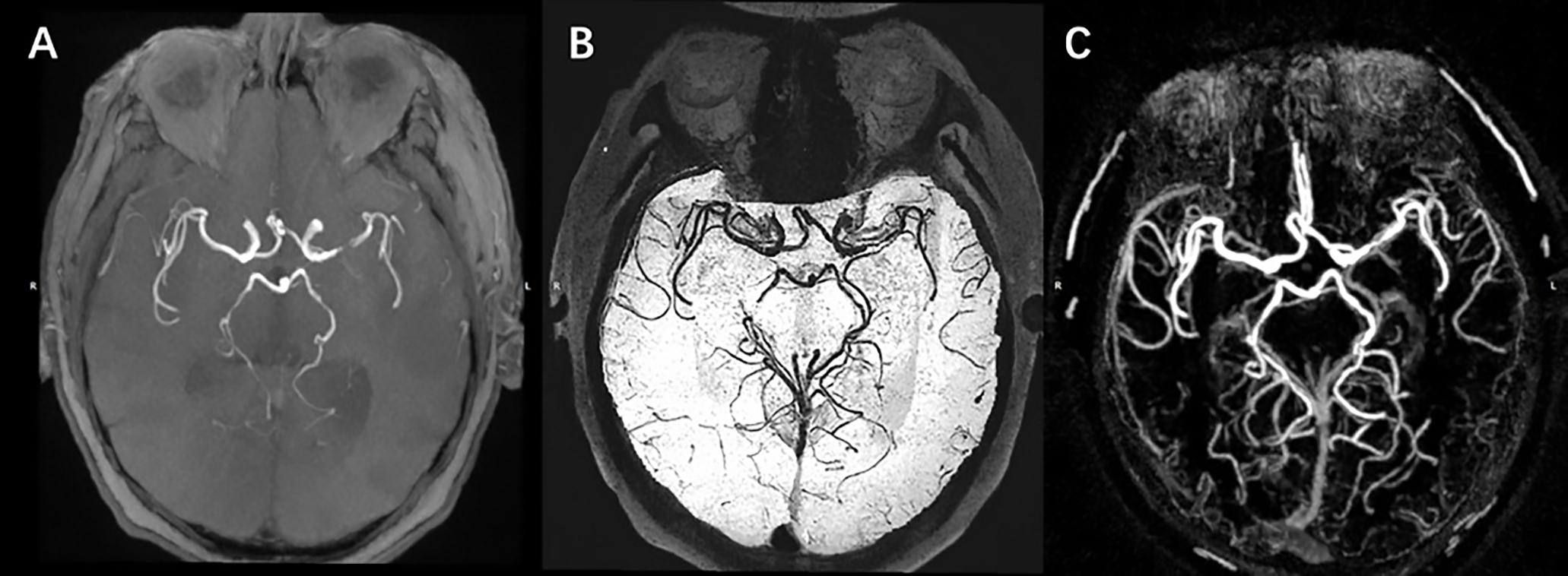
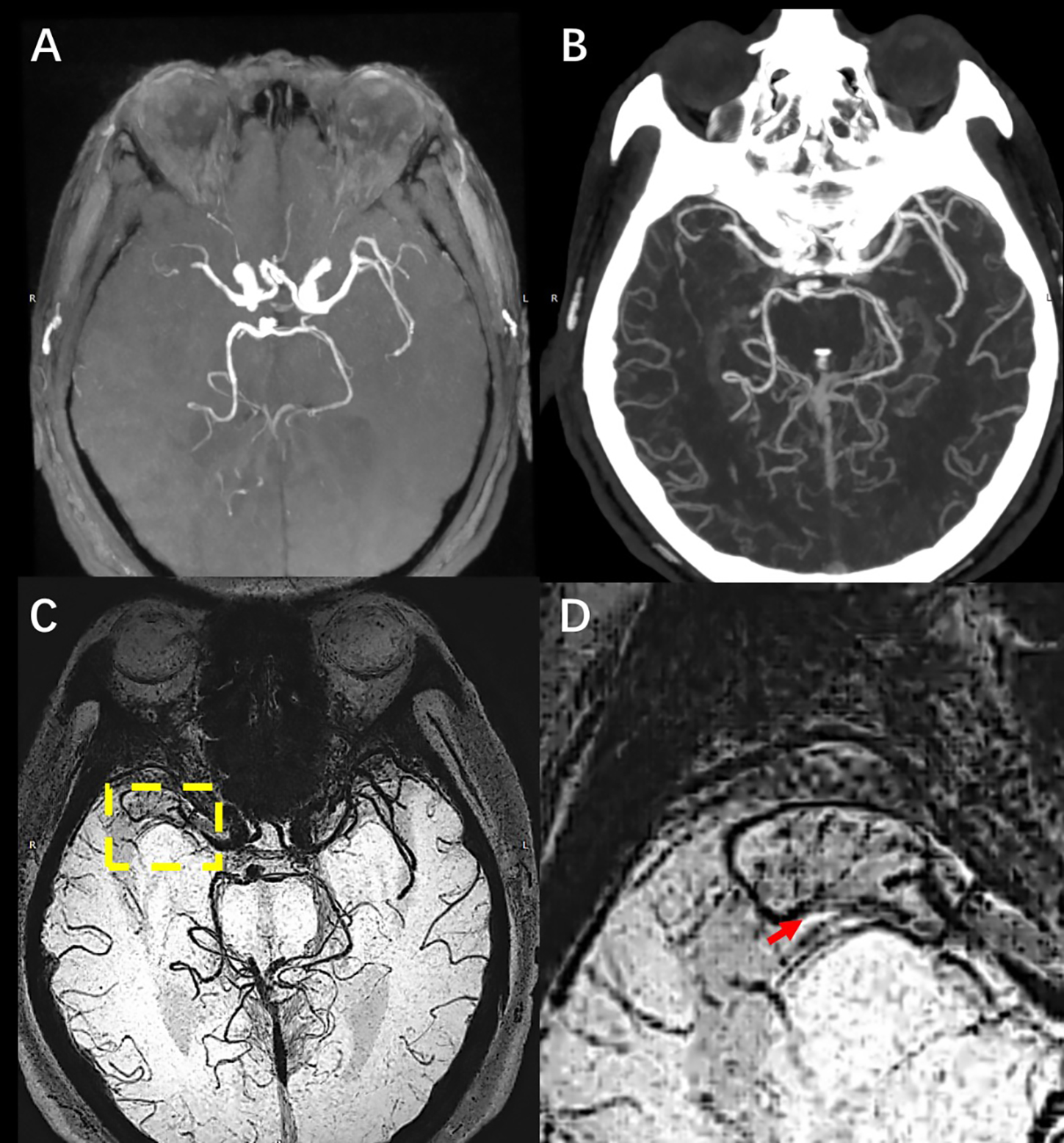
Stenosis, distal branches and collateral circulation were of great importance in assessing vulnerable vessel beds in stroke patients. Minimum intensity projection(mIP) MRA was derived from high resolution vessel wall imaging (HR VWI), which can be used as evaluating vessel wall, as well as vessel lumen. At present, researches on intracranial small vessels based on mIP MRA concentrate on lenticulostriate arteries[1, 2]. However, steno-occlusive MCA and its distal leptomeningeal branches were not studied. This study aims to assess the feasibility of mIP MRA of HR VWI for evaluating MCA stenosis, occlusion, accompanying microvascular (AMV) and leptomeningeal branches.Methods
This retrospective study included 20 patients with MCA territory acute ischemic stroke. All patients completed intracranial CTA, TOF MRA and HR VWI. HR VWI was scanned with PDw SPACE sequence using a 3.0T scanner (Trio-Tim, SiemensHealthcare, Erlangen). mIP MRA was generated by performing minimal intensity projection on the transvers PDw SPACE. MCA stenosis, occlusion, AMV and leptomeningeal branches in M1 to M3 according to Alberta Stroke Program Early CT Score (ASPECTS) were recorded respectively on the above three imaging techniques (CTA, TOF MRA and mIP MRA). The sensitivity, specificity, diagnostic coincidence rate (DCR), positive predictive value (PPV), negative predictive value (NPV), Youden index (YI) and accuracy of TOF MRA and mIP MRA were calculated, with CTA as the standard reference.Results
Mild to moderate stenosis was in excellent agreement between TOF MRA and CTA (Kappa=0.843), while severe stenosis and occlusion tended to be overestimated (Kappa=0.709 vs Kappa=0.643). Mild to moderate stenosis, severe stenosis, and occlusion showed complete agreement between mIP MRA and CTA (Kappa=1). Compared with CTA, the sensitivity of AMV, leptomeningeal branches in regional M1 to M3 according to ASPECTS were low (less than 30%), and of poor agreement (Kappa<0.4). All the sensitivity, specificity, DCR, PPV, NPV, YI and accuracy of mIP were larger than 90%. Leptomeningeal branches in ASPECTS M3 was in fair agreement between mIP MRA and CTA (Kappa=0.481), while all the other index were in excellent agreement (Kappa>0.75). The DCR, YI and agreement between mIP MRA and CTA were higher than TOF MRA.Conclusion
Using CTA as a standard, mIP MRA outperformed TOF MRA in assessing MCA stenosis, occlusion, AMV and leptomeningeal branches. Consistent with CTA, mIP MRA is feasible for clinical application, and may help in detecting collaterals.Acknowledgements
This work was supported by NSFC-NIH (81361120402) .References
1. Zhang Z, Fan Z, Kong Q, et al. Visualization of the lenticulostriate arteries at 3T using black-blood T1-weighted intracranial vessel wall imaging: comparison with 7T TOF-MRA. Eur Radiol. 2018;27:1-8.
2. Liang J, Liu Y, Xu X, Shi C, Luo L. Cerebral Perforating Artery Disease. Clin Neuroradiol. 2018;23:1-9.
Figures