2060
Improved vessel delineation in whole-heart coronary MRA with sub-millimeter isotropic resolution using deep learning reconstruction compared with routine whole-heart coronary MRA1Kyorin University Hospital, Tokyo, Japan, 2Kyorin University School of Medicine, Tokyo, Japan, 3CANON MEDICAL SYSTEMS CORPORATION, Otawara, Japan
Synopsis
Whole-heart coronary MRA (WHCMRA) with sub-millimeter isotropic resolution is expected to improve spatial resolution and overcome limitations of routine WHCMRA, whereas increased image noise is the drawback. A state-of-the-art 3T MR scanner with the maximal gradient magnetic field of 100 mT/m and capability of deep learning reconstruction (DLR) that aims to reduce image noise is useful for improving vessel sharpness and delineation of the coronary arteries, even in the distal segments, on WHCMRA with sub-millimeter isotropic resolution with use of the DLR with preserving image noise compared with routine WHCMRA.
Introduction
Three-dimensional whole-heart coronary MRA (WHCMRA) allows noninvasive morphological assessment of coronary artery disease without radiation exposure or contrast media administration. Conventional WHCMRA has been limited in delineation of distal coronary segments and quantification of vessel lumen stenosis due to its insufficient spatial resolution. WHCMRA with sub-millimeter isotropic resolution is required to overcome these limitations with improving the spatial resolution1. Recently, a state-of-the-art 3T MR scanner (Vantage Galan 3T/ZGO; Canon, Tochigi, Japan) with the maximal gradient magnetic field of 100 mT/m and capability of deep learning reconstruction (DLR) that aims to reduce image noise in every scanned region has been clinically introduced. Without degrading image interpretability, use of the DLR can improve vessel delineation on the WHCMRA with sub-millimeter isotropic resolution acquired with this MR scanner. The purpose of the present study was to assess the usefulness of the WHCMRA with sub-millimeter isotropic resolution with the DLR for improving vessel delineation compared with routine WHCMRA.Methods
With this MR scanner, 10 healthy volunteers (9 men and 1 woman; mean age, 37 ± 8 years; range, 26 to 53 years) underwent ECG- and respiration-gated WHCMRA with isotropic 0.9 x 0.9 x 0.9 mm3 resolution with and without the DLR and routine WHCMRA with anisotropic 1.2 x 1.6 x 1.7 mm3 resolution without the DLR using the following scan parameters: TE, 1.9 msec; TR, 5 msec; flip angle, 12 degrees; FOV, 30 cm. We reconstructed their axial and curved multiplanar reformation images and placed regions of interest (ROIs) in the interventricular septum to measure the standard deviation (SD) of its signal intensity as the background noise on all the WHCMRA images (Figure 1). The full width at half maximum (FWHM) of the lumen diameter of the proximal segment of the right coronary (RCA) or left circumflex arteries (LCX) was measured on the WHCMRA with sub-millimeter isotropic resolution with the DLR and routine WHCMRA in each volunteer (Figure 2). Two readers by consensus visually graded image quality (IQ) regarding vessel sharpness and delineation in the proximal to middle segments and the distal segments of the RCA, left anterior descending artery (LAD), and LCX using a five-point scale (one, poor; five, excellent) (Figure 3). We used ANOVA and Bonferroni tests to compare the background noise among the WHCMRA with sub-millimeter isotropic resolution with and without the DLR and routine WHCMRA and paired t test to compare the FWHM and Wilcoxon signed rank test to compare the IQ in both the proximal to middle segments and the distal segments of the three vessels between the WHCMRA with sub-millimeter isotropic resolution with the DLR and routine WHCMRA.Results
The background noise was significantly higher on the WHCMRA with sub-millimeter isotropic resolution without the DLR (43.3 ± 13.1) than on the WHCMRA with sub-millimeter isotropic resolution with the DLR (27.1 ± 5.2) and routine WHCMRA (20.3 ± 6.9) (P = 0.001 and <0.001, respectively) and comparable between the last two (P = 0.304). Other results of this study are shown in Table 1. The FWHM was significantly lower on the WHCMRA with sub-millimeter isotropic resolution with the DLR than on the routine WHCMRA. The IQ was significantly better in both the segments of all the three vessels on the WHCMRA with sub-millimeter isotropic resolution with the DLR than on the routine WHCMRA.Discussion
The WHCMRA with sub-millimeter isotropic resolution with the DLR well delineated all the three vessels, even in the distal segments, as shown in Figure 4. Although increased image noise is a drawback of the WHCMRA with sub-millimeter isotropic resolution, use of the DLR can decrease image noise and improve the IQ of the coronary arteries. Thus, this WHCMRA can be a good alternative to coronary CTA for noninvasive morphological assessment of coronary artery disease for patients in whom coronary CTA is not indicated for reasons including iodine allergy and renal insufficiency.Conclusion
The WHCMRA with sub-millimeter isotropic resolution with the DLR is useful for improving vessel sharpness and delineation of the coronary arteries with preserving image noise compared with the routine WHCMRA.Acknowledgements
No acknowledgement found.References
1. Bustin A, Ginami G, Cruz G, et al. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn Reson Med 2018 Jul 29. doi: 10.1002/mrm.27354. [Epub ahead of print]Figures

Figure 1
Axial images of WHCMRA with sub-millimeter isotropic resolution with (a) and without DLR (b) and routine WHCMRA (c) with circular ROIs placed in the interventricular septum to measure the background noise (SD) (a-c, the yellow circles). Vessel sharpness of RCA, LAD, and LCX (a-c, the yellow arrows) is better on WHCMRA with sub-millimeter isotropic resolution with (a) and without DLR (b) than routine WHCMRA (c). The noise is higher on WHCMRA with sub-millimeter isotropic resolution without DLR (b) than on WHCMRA with sub-millimeter isotropic resolution with DLR (a) and routine WHCMRA (c) and comparable between the last two.

Figure 2
Axial images of WHCMRA with sub-millimeter isotropic resolution with DLR (a) and routine WHCMRA (b) with FWHM measurements in the proximal segment of RCA. The FWHM is lower on WHCMRA with sub-millimeter isotropic resolution with DLR (a, 2.6 mm) than on routine WHCMRA (b, 2.9 mm).
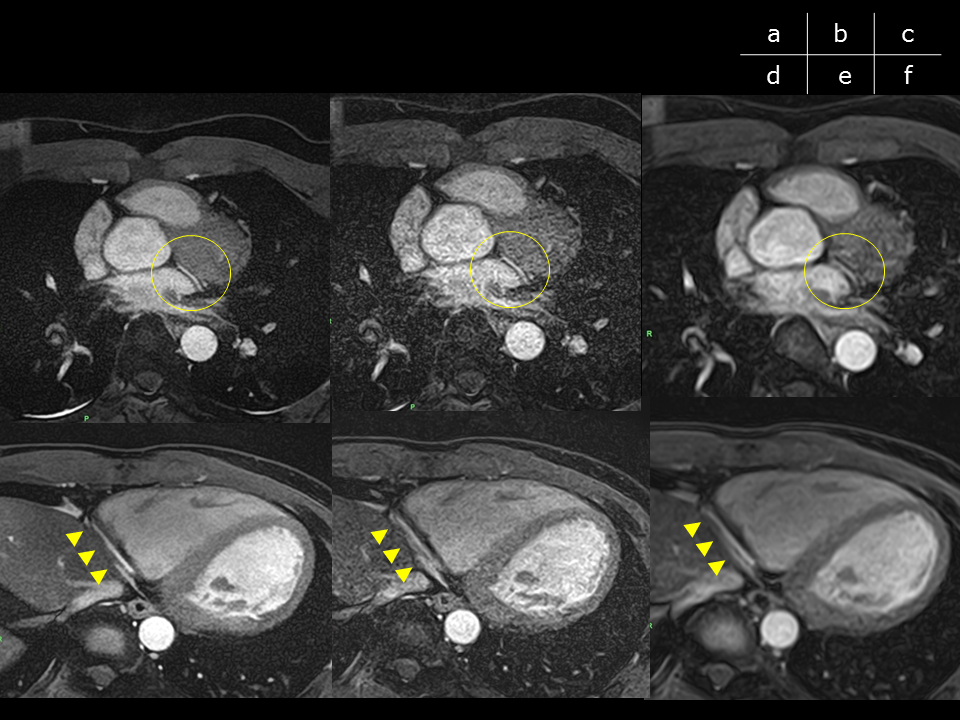
Figure 3
Axial images of WHCMRA with sub-millimeter isotropic resolution with (a, d) and without DLR (b, e) and routine WHCMRA (c, f). Vessel sharpness in the proximal segment of LCX (a-c, the yellow circle) and the distal segment of RCA (d-f, the yellow arrowheads) are better on WHCMRA with sub-millimeter isotropic resolution with (a, d) and without DLR (b, e) than routine WHCMRA (c, f). The vessel delineation on WHCMRA with sub-millimeter isotropic resolution is better with DLR (a, d) than without DLR (b, e).

Table 1
Results of the present study. The FWHM of the lumen diameter of the proximal segment of RCA or LCX and IQ in the proximal to middle segments and the distal segments of RCA, LAD, and LCX are compared between WHCMRA with sub-millimeter isotropic resolution with DLR and routine WHCMRA.
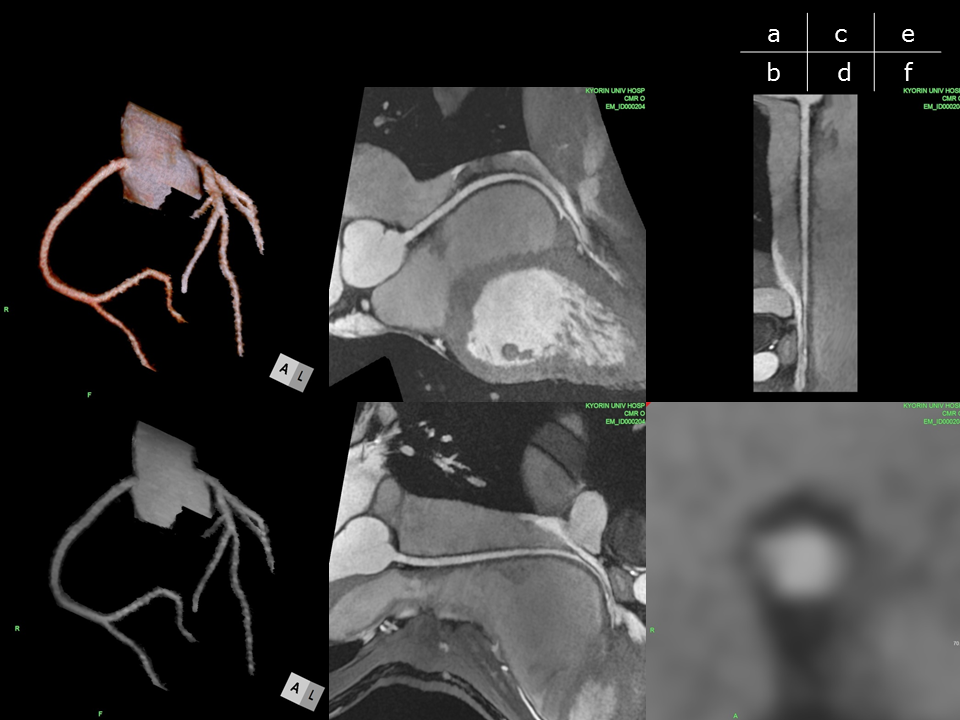
Figure 4
Volume-rendered (a) and maximum intensity projection images of WHCMRA with sub-millimeter isotropic resolution with DLR (b) and its curved multiplanar reformation images of RCA (c-f) including the stretched (e) and short-axis views (f). These images well delineate all the coronary vessels, even in their distal segments, with the improved vessel sharpness and signal homogeneity like coronary CTA.