2059
Radial self-navigated non contrast-enhanced (CE-) MRA in comparison to conventional navigator-gated CE-MRA of the thoracic aorta in a vascular patient collective1Department of Diagnostic, Interventional and Pediatric Radiology, Inselspital, University of Bern, Bern, Switzerland, 2Department of Radiology, UH Cleveland Medical Center, Cleveland, USA, Cleveland, OH, United States, 3Advanced Clinical Imaging Technology, Siemens Healthcare, Lausanne, Switzerland, Bern, Switzerland, 4Department of Radiology, University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, Lausanne, Switzerland
Synopsis
This study compares a conventional Cartesian contrast-enhanced MRA sequence with a native 3D radial MRA sequence for imaging the aortic root and the ascending aorta. The difference in image quality between those two MRA sequences has been shown to be highly significant at the ascending aorta and the aortic arch with higher quality for the radial self-navigated non-contrast enhanced MRA. The results of our study support the potential of a native MRA protocol as a diagnostic tool in monitoring the geometry or size of the aortic root and the ascending aorta.
Introduction
High resolution magnetic resonance angiography (MRA) of the thoracic aorta is important for therapy planning in aortic valve implantation or follow up of vascular patients. Cardiac and breathing motion may hamper image quality in the aortic root and the ascending thoracic aorta. Contrast-enhanced (CE) MRA is a well established technique for robust and fast visualization of vessels1. However, in vascular patients with compromised renal function, the use of non CE-MRA such as bSSFP-based angiography techniques is favored2,3. Compared to Cartesian data acquisition radial trajectories are less prone to motion artifacts. Recently, a radial self-navigated method based on a bSSFP sequence has been introduced for imaging the coronary arteries that do not require the use of contrast agent4. Whereas navigator respiration control often results in unpredictable scan times, self-navigation based on an inherent signal that allows a correction of different breathing motion states provides a data efficiency of 100%. The purpose of this study was to compare a conventional Cartesian first-pass CE-MRA sequence with a native 3D radial self-navigated MRA sequence in terms of image quality parameters.Methods
In this IRB approved study, a total of 92 vascular patients (mean age=63.5 years) were enrolled into the study receiving the MR examination for clinical indication. Radial self-navigated MRA included 31 patients (mean age=64 years) and first-pass CE-MRA 61 patients (mean age=63 years). All measurements were performed on a 1.5T scanner (Magnetom Aera, Siemens, Healthcare, Erlangen, Germany). The imaging protocol consisted of the following major sequences: A native MRA based on an ECG-triggered self-navigated 3D radial bSSFP sequence (TA=3 min 20 s) was acquired with an inherent isotropic FOV of 25cm and spatial resolution of 1.3mm4. Next, a time-resolved CE-MRA was performed with 0.2ml/kg body weight Multihance (½dose) at flow rate 2.5ml/s providing the bolus arrival time of the contrast agent. Finally, an ECG-triggered first-pass gradient-echo based CE-MRA with navigator respiration control (TA= 5 min 44 s) was acquired with a FOV of 34×25.5×8.3cm and a spatial resolution of 1.4×1.3×1.3mm, using 0.2ml/kg body weight Multihance (½dose) at flow rate of 0.4ml/s. Image quality of the two different MRA sequences was assessed by visual analysis of vessel contrast (lumen versus vessel wall), sharpness of vessel wall and artifacts. All evaluations were performed by two readers each with 7 years of experience. A grading as following was defined. 1: Excellent vessel definition without blurring; 2: good definition with mild blurring; 3: moderate definition with substantial blurring; 4: non-diagnostic due to severe artifacts. Three aortic locations (ascending aorta, aortic arch, descending aorta) were used for grading. To measure the inter-rater agreement Cohen`s kappa coefficient (κ) was calculated. To assess statistical differences between the two MRA sequences, the 4-point scale consensus ratings were re-coded to achieve binary ratings (“excellent/good” versus “moderate/poor”) and a Chi-squared test was applied.Results
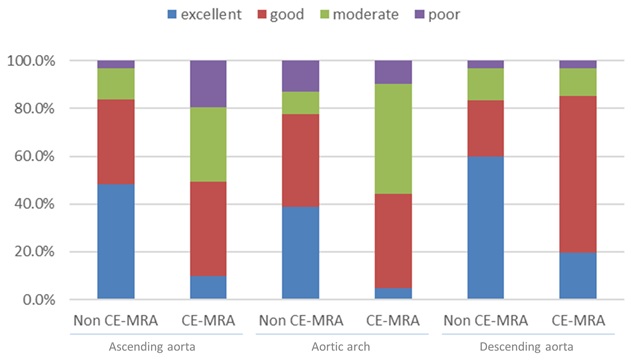
The inter-rater agreement was (κ)=0.96, which corresponds to an excellent agreement. At the ascending aorta image quality was rated excellent in 48%, good in 36%, moderate in 13% and poor in 3% for radial self-navigated non CE-MRA, and excellent in 10%, good in 39%, moderate in 31% and poor in 20% for CE- MRA, respectively. The visualization of the aortic arch was rated excellent in 39%, good in 39%, moderate in 10% and poor in 13% for radial self-navigated non CE-MRA and excellent in 5%, good in 39%, moderate in 46% and poor in 10% for CE-MRA, respectively (Table and Figure 1). In a comparison of non CE-MRA versus CE-MRA, the ascending aorta and the aortic arch showed a highly significant difference (p=0.00127 and p=0.00249, respectively). No significant difference was shown at the descending aorta (p=0.81) due to the absence of pronounced motion effects.Discussion
This study revealed a highly significant higher image quality in the ascending aorta and in the aortic arch in radial self-navigated MRA without contrast media application compared to Cartesian first-pass CE-MRA. The self-navigated non CE- MRA comes along with a clearly reduced scan time compared to the navigator-gated CE-MRA. The poor image quality was mostly due to motion and susceptibility artifacts, as vascular patients predominantly with foreign material implants were analyzed. A detailed analysis of how the presence of foreign materials like sternal cerclage or artificial heart valves deteriorates image quality for different MRA methods is of interest for future work. In conclusion diagnostic image quality of the thoracic aorta can be obtained without administration of contrast media offering a benefit in potential side effects of contrast media, especially in patients with impaired renal function or by avoiding deposition of Gd in the body in general.Acknowledgements
The authors thank all the involved members of the study and all the MR technologists for their valuable participation, helpfulness, and supportduring this study.References
1. Liu Q et al. Three-dimensional contrast-enhanced MR angiography of aortic dissection: a pictorial essay. Radiographics 2007; 27: 1311–1321.
2. Di Cesare E et al. CT and MR imaging of the thoracic aorta. Open Med (Wars) 2016;11:143-151.
3. Von Tengg-Kobligk H et al. Imaging modalities for the thoracic aorta. J Cardiovasc Surg 2008;49:429-47.
4. Piccini D et al. Respiratory self‐navigation for whole‐heart bright‐blood coronary MRI: Methods for robust isolation and automatic segmentation of the blood pool. Magn Reson Med 2012;68:571-9.
Figures