2057
Ultrashort TE Time-Spatial Labeling Inversion Pulse MR Angiography Denoised with Deep Learning Reconstruction for Abdominal Visceral Arteries: A Feasibility Study1Department of Radiology, Tohoku University Hospital, Sendai, Japan, 2Diagnostic Radiology, Tohoku University Hospital, Sendai, Japan, 3Canon Medical Systems corp., Tochigi, Japan
Synopsis
We have developed ultrashort TE (UTE) time-SLIP MRA for the evaluation of abdominal visceral arteries. In this volunteer study, although image quality and number of visualized renal arteries on UTE time-SLIP MRA were inferior to those on steady-state free precession (SSFP) time-SLIP MRA, deep learning reconstruction enabled significant improvement of signal-to-noise ratio and contrast to the background tissue. In patients with visceral artery aneurysms treated by endovascular intervention, contrast ratio of treated segment adjacent to metal devices to the aorta were higher on UTE than SSFP time-SLIP MRA. This proposed technique is feasible for visceral artery disease after endovascular interventions.
Introduction
Non-contrast time-spatial Labeling Inversion Pulse (time-SLIP) MRA using steady-state free precession (SSFP) technique is currently accepted for the evaluation of abdominal visceral vessels (1, 2). Although SSFP provides a high signal efficiency with intrinsic T2/T1 contrast for luminal visualization, there are potentially degrading factors including intravoxel dephasing from accelerated blood flow in the stenosis, turbulent flow and susceptibility artifacts caused by metallic devices. Motion artifacts caused by the irregular respiration may result in suboptimal image quality. Ultrashort TE (UTE) based MRA was introduced to assess intracranial arteries treated by coils and stents (3, 4). It provided better visualization of in-stent flow than time-of-flight MRA. Its radial sampling scheme is tolerant of motion. In this study, UTE time-SLIP MRA technique has been developed to potentially be applied for the evaluation of visceral arteries after endovascular interventions. We aimed to evaluate the feasibility of UTE time-SLIP MRA for abdominal visceral arteries by comparing with SSFP time-SLIP MRA. The values of this denoising approach with deep learning reconstruction (dDLR) were evaluated for both imaging technique.Methods
The local institutional review board approved this prospective study. A total of 10 healthy subjects (7 men, mean age, 30 ± 7.5 years, range 23–50) and five patients with visceral artery aneurysms treated by endovascular interventions were enrolled. All subjects underwent non-contrast time-SLIP MRAs (UTE and SSFP) on a 3T MR scanner (Vantage, Titan 3T, Canon Medical Systems, Tochigi, Japan). UTE time-SLIP MRA was acquired with 3.7ms TR, 0.096ms TE, 5 degrees of flip angle, 9960 of trajectory, 120 segments, 1500ms of BBTI, 1.29mm*1.29mm*2mm of spatial resolution. SSFP time-SLIP MRA was acquired with 4.8ms TR, 2.4ms TE, 66 degrees of flip angle, 1500ms of BBTI, 1.29mm*1.29mm*2mm of spatial resolution. All Acquired data was reconstructed with and without dDLR.
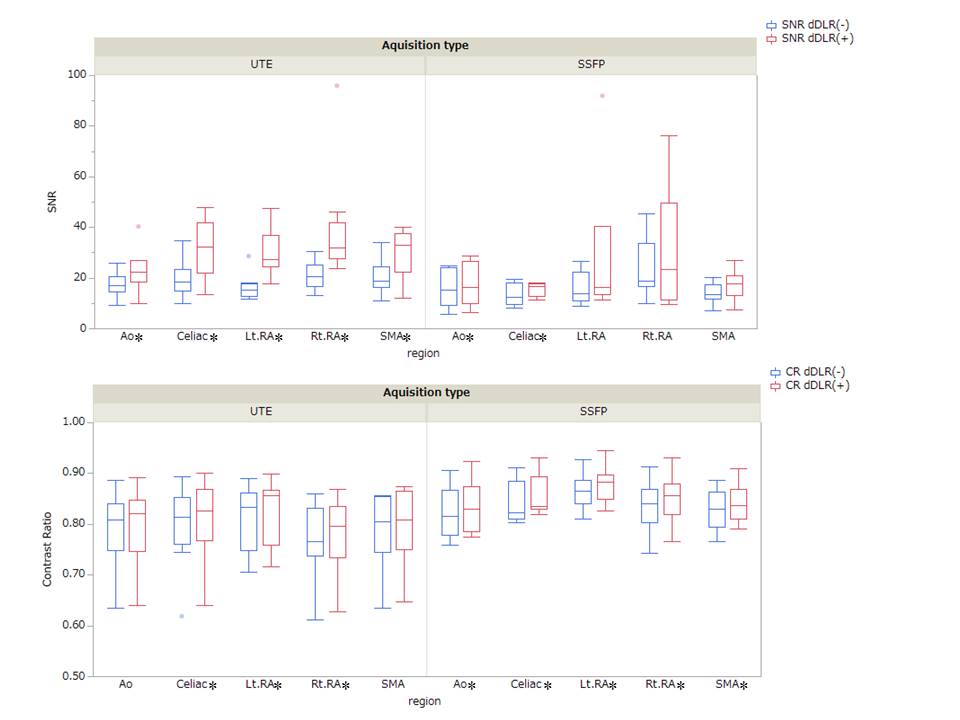
Volunteer study: Two reviewers evaluated 4 sets of images in consensus reading. Regions of interests were placed to measure local signal-to-noise ratio (SNR) of the aorta, celiac artery, superior mesenteric artery and renal arteries as well as contrast ratio (CR) of each vessel to the visceral fat tissue. The ordinal number of visualized renal arterial branches and a five-point image quality score (1, poor, 5, excellent) were evaluated.
Patient study: CR of the patent arterial segment adjacent to platinum coils (n=3) or inside nitinol stents (n=2) to the aorta (CRseg) were evaluated for both MRAs with dDLR.
Statistical analysis: Wilcoxon signed-rank tests were used to compare variables between two image data sets. a p value < 0.05 was considered to be statistically significant.
Results
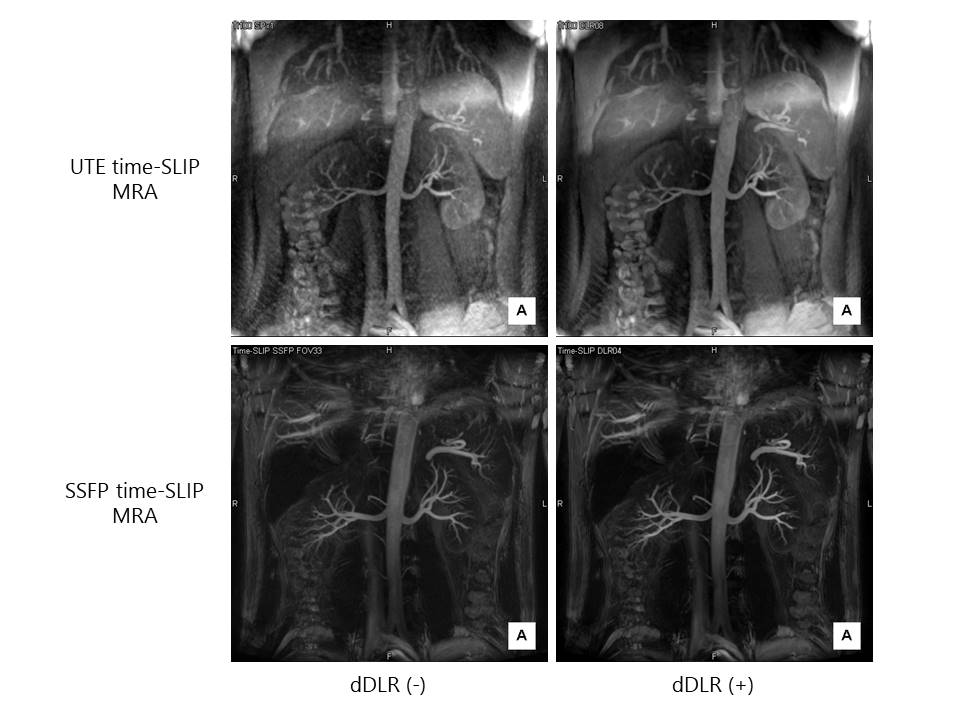
Volunteer study: dDLR significantly improved SNR of all the segments on UTE time-SLIP MRA and that of the aorta and celiac artery on SSFP time-SLIP MRA (fig. 1, 2). dDLR also significantly improved CR of branch arteries on both MRAs except for the superior mesenteric artery on UTE time-SLIP MRA (fig. 1, 2). The mean ordinal number of visualized renal arterial branches was lower on UTE time-SLIP MRA than the other (2.75 vs. 3.5, p<0.01), which was the same when those with dDLR when compared. dDLR improved visual image quality scores on UTE time-SLIP MRA (2.6 without dDLR vs 3.2 with dDLR, p < 0.01), but not on SSFP time-SLIP MRA (4.1 vs. 4.0, p=0.48).
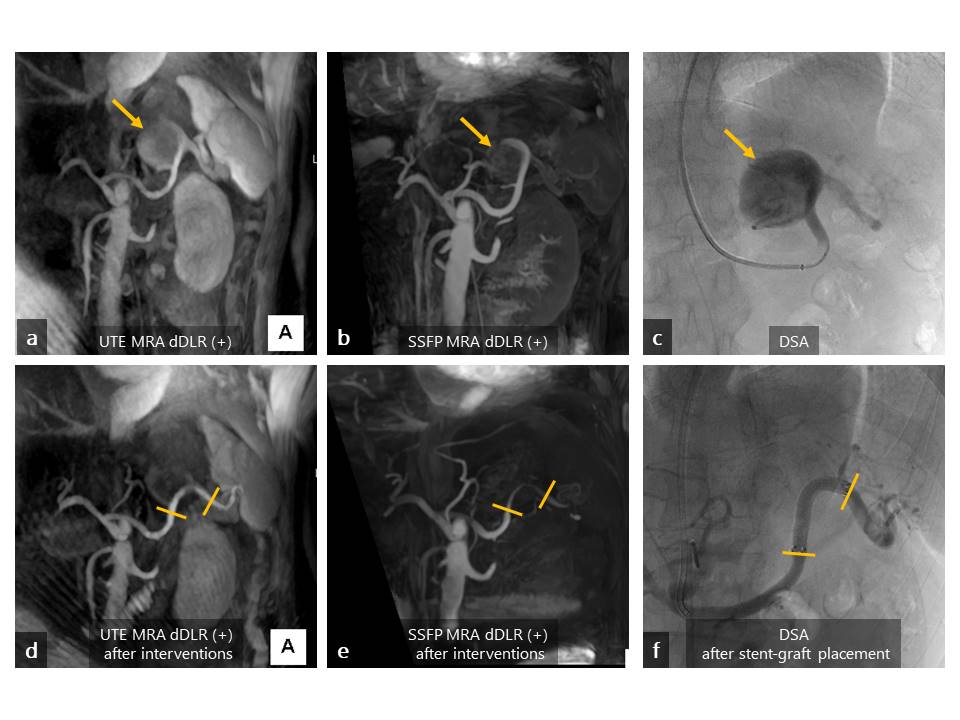
Patient study: In all patients, CRseg was higher on UTE time-SLIP MRA than the other (p < 0.043). Especially, signals of in-sent patent segments in the splenic arteries of the two patients were better visualized on UTE than SSFP time-SLIP MRA (fig. 3).
Discussion and Conclusion
In time-SLIP MRA technique, suppression of background signal including visceral fat and organs were desired to better depict target arteries. dDLR worked for significant reduction of image noise, contributing to improvement of SNR and CR, especially in the branch arteries. A potential limitation of UTE MRA due to streak artifacts and residual background signal noises has been overcome with dDLR, resulting in significant improvement of image quality scores. On the other hand, the image quality score was not improved with dDLR on SSFP time-SLIP MRA, probably because original score without dDLR was already high. Using dDLR, the advantage of UTE technique against signal decay adjacent to metal devises was enhanced. Further optimization of parameters will be required to eliminate streak artifacts including number of trajectories for the UTE acquisition. In conclusion, the newly developed UTE time-SLIP MRA with dDLR is feasible to evaluate patients with visceral arterial diseases treated by endovascular interventions.Acknowledgements
We thank Mr. Yuichi Yamashita, Canon Medical Systems Corp., for the support of this study.References
1. Albert TSE, Akahane M, Parienty I, et al.: An International Multicenter Comparison of Time-SLIP Unenhanced MR Angiography and Contrast-Enhanced CT Angiography for Assessing Renal Artery Stenosis: The Renal Artery Contrast-Free Trial. Am J Roentgenol 2014; 204:182–188. 2. Brucher N, Vial J, Baunin C, et al.: Non-contrast-enhanced MR angiography using time-spin labelling inversion pulse technique for detecting crossing renal vessels in children with symptomatic ureteropelvic junction obstruction: comparison with surgical findings. Eur Radiol 2016; 26:2697–2704. 3. Irie R, Suzuki M, Yamamoto M, et al.: Assessing Blood Flow in an Intracranial Stent: A Feasibility Study of MR Angiography Using a Silent Scan after Stent-Assisted Coil Embolization for Anterior Circulation Aneurysms. AJNR Am J Neuroradiol 2015; 36:967–970. 4. Takano N, Suzuki M, Irie R, et al.: Usefulness of Non–Contrast-Enhanced MR Angiography Using a Silent Scan for Follow-Up after Y-Configuration Stent-Assisted Coil Embolization for Basilar Tip Aneurysms. Am J Neuroradiol 2017; 38:577–581.Figures