2056
Direct and Indirect Signs of Pulmonary Embolism at MRA: Inter and Intra Reader Agreement1Radiology, University of Wisconsin - Madison, Madison, WI, United States, 2Radiology, University of Arkansas for Medical Sciences, Little Rock, AR, United States
Synopsis
Direct and indirect finding of pulmonary embolism are important for making the correct diagnosis on pulmonary MRA. We have assessed the prevalence of both expected direct and indirect findings of PE and also evaluated the inter and intra reader agreement of these indirect and direct findings. Our results demonstrate that experienced and inexperienced observers can reproducibly observe direct and indirect findings of PE on CEMRA exams.
INTRODUCTION:
Computed tomography pulmonary angiography (CTPA) is currently the imaging standard of care for the diagnosis of PE1. CTPA can be performed and interpreted rapidly, resulting in its widespread use in the emergency setting. However, CTPA has its limitations including increasing concerns about the effects of ionizing radiation, particularly for younger women2-4. Also, some patients have contraindications to iodinated contrast, including those with renal failure or a history of allergic or anaphylactoid reaction to the contrast material.
Contrast enhanced magnetic resonance angiography (CE-MRA) is being used increasingly for the primary diagnosis of PE and does not require either iodinated contrast or ionizing radiation5-8. Accurate diagnosis of PE requires the interpreting radiologist to be aware of both the direct and indirect findings that can be seen on CE-MRA in patients with PE. Many of these findings can also be seen in CTPA, while others are unique to CE-MRA.
The purpose of this study is to determine the inter and intra reader agreement and prevalence of various direct and indirect signs of pulmonary embolism (PE) on contrast enhanced pulmonary magnetic resonance angiography (CE-MRA).
METHODS:
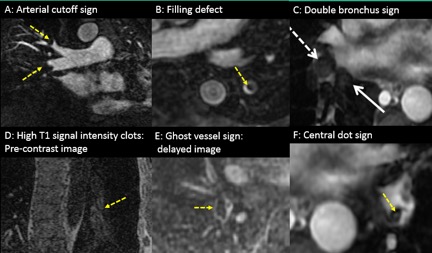
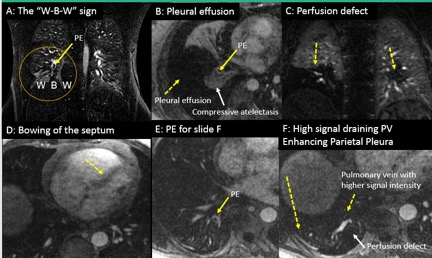
This was a HIPPA compliant and IRB approved retrospective study of PE positive CE-MRA exams. The direct signs that were evaluated included the following: occlusive and non-occlusive filling defects, vessel cutoff, double bronchus sign, central dot, ghost vessel, high T1 signal clot and visibility on post-contrast T1 with fat saturation. The indirect findings evaluated included: perfusion defect, white-black-white interface, blank slate, pleural enhancement, pleural effusion, pulmonary infarction, pulmonary venous stasis and atelectasis. Examples of the direct and indirect findings are shown in Figures 1 and 2, respectively. Studies were interpreted twice by two readers and each pulmonary embolus was individually graded. Reader 1 had 2 years of experience interpreting MRA for PE while Reader 2 had 6 weeks of experience. Each reading was performed at least one week apart to prevent recall bias. Cohen’s kappa test determined the inter and intra reader agreement for each sign. A p value of 0.05 determined statistical significance.RESULTS:
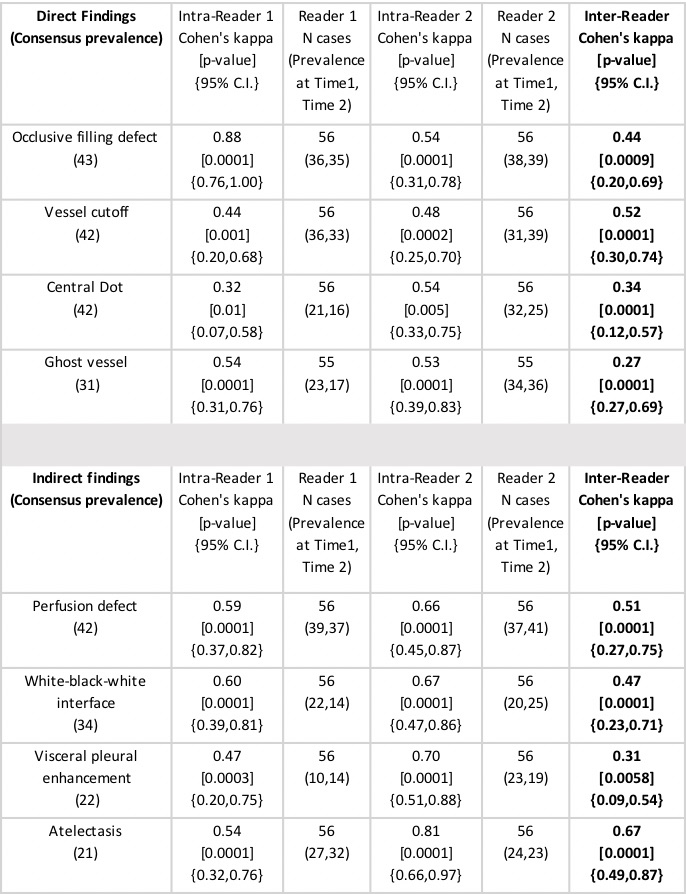
We reviewed 66 positive CE-MRA exams. We used 10 cases for training. The largest PE for each of the remaining 56 cases were included in this analysis. The prevalence, intra reader and inter reader agreement for the most reproducible direct and indirect findings are shown in Figure 3. We found that the two most prevalent direct findings of PE were the occlusive filling defect and vessel cutoff. The two most prevalent indirect signs were perfusion defects and the white-black-white interface. The inter reader agreement for these two direct findings was average (k = 0.44 and k=0.52) and the agreement for these two indirect findings was good (k = 0.51 and 0.47).DISCUSSION:
Contrast enhanced magnetic resonance imaging (CE-MRA) is becoming an increasingly important modality for detecting pulmonary embolism (PE) especially in those situations where there are concerns about excess exposure to ionizing radiation or contraindications to iodinated contrast. While most radiologists are experienced in interpreting pulmonary computed tomography angiographic (CE-MRA) studies, many are uncomfortable performing and interpreting pulmonary CE-MRA. When a high-quality exam is performed, large PE can easily be seen directly. When the quality of the exam is limited, or the PE is small, knowledge of indirect findings can assist in localizing PE or determining its likely presence.CONCLUSION:
Experienced and inexperienced observers can reproducibly observe direct and indirect findings of PE on CE-MRA exams.Acknowledgements
Support for this research was provided by General Electric.References
1. Stein PD, Fowler SE, Goodman LR, et al. Multidetector computed tomography for acute pulmonary embolism. N Engl J Med. 2006;354(22):2317-27.2.
2. Brenner DJ, Hall EJ. Computed tomography--an increasing source of radiation exposure. N Engl J Med. 2007;357(22):2277-84.3.
3. Hall EJ, Brenner DJ. Cancer risks from diagnostic radiology: the impact of new epidemiological data. Br J Radiol. 2012;85(1020):e1316-7.4.
4. Pearce MS, Salotti JA, Little MP, et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet. 2012;380(9840):499-505.5.
5. Schiebler ML, Nagle SK, Francois CJ, et al. Effectiveness of MR angiography for the primary diagnosis of acute pulmonary embolism: clinical outcomes at 3 months and 1 year. Journal of magnetic resonance imaging : JMRI. 2013;38(4):914-25.6.
6. Repplinger MD, Nagle SK, Harringa JB, et al. Clinical outcomes after magnetic resonance angiography (MRA) versus computed tomographic angiography (CTA) for pulmonary embolism evaluation. Emerg Radiol. 2018 Oct;25(5):469-477.7.
7. Benson DG, Schiebler ML, Repplinger MD, et al. Contrast-enhanced pulmonary MRA for the primary diagnosis of pulmonary embolism: current state of the art and future directions. Br J Radiol. 2017 Jun;90(1074):20160901.8.
8. Benson DG, Schiebler ML, Nagle SK, François CJ. Magnetic Resonance Imaging for the Evaluation of Pulmonary Embolism. Top Magn Reson Imaging. 2017 Aug;26(4):145-151
Figures