2054
Comparison of Gadolinium- and Ferumoxytol- enhanced Conventional and ultra-short echo time MR-Angiography for the Depiction of the Pulmonary Vasculature1Radiology, University of Wisconsin – School of Medicine and Public Health, Madison, WI, United States, 2Medical Physics, University of Wisconsin – School of Medicine and Public Health, Madison, WI, United States, 3Biomedical Engineering, University of Wisconsin – School of Medicine and Public Health, Madison, WI, United States, 4Medicine, University of Wisconsin – School of Medicine and Public Health, Madison, WI, United States, 5Emergency Medicine, University of Wisconsin – School of Medicine and Public Health, Madison, WI, United States, 6Pediatrics, University of Wisconsin – School of Medicine and Public Health, Madison, WI, United States
Synopsis
Pulmonary MRA is a promising technique for detection
of pulmonary embolism without ionizing radiation. Unfortunately, a subset of
patients fail breath-holding during conventional MRA (cMRA). Free-breathing ultra-short
echo time (UTE)-MRA could overcome this limitation but would require a blood
pool contrast agent due to longer scan times. Ferumoxytol (FE) can be used as
an off-label MR-contrast agent with a blood half-life of 10-14 hours. This study
compared gadobenate dimeglumine (GD)-enhanced-UTE-MRA to FE-cMRA and FE-UTE-MRA,
using GD-cMRA as reference standard. Results suggest that FE-UTE-MRA has
improved performance compared to GD-cMRA for depicting non-vascular structures while
offering excellent angiographic image quality.
Introduction
Conventional pulmonary MRA (cMRA) is an attractive alternative to CTA for diagnosis of pulmonary embolism (PE) but shows inferior depiction of the lung parenchyma1-3 and may be limited in dyspneic patients that fail the breath-holding. Free-breathing ultra-short echo time (UTE)-MRA could overcome these limitations but would require a blood pool CA due to longer scan times. Ferumoxytol (FE) can be used as an off-label MR-contrast agent with favorable T1-shortening properties4 and a blood half-life of 10-14 hours. The purpose of this study was 1) to evaluate the feasibility of three new approaches: gadobenate dimeglumine (GD)-enhanced UTE-MRA, FE-UTE-MRA, and FE-cMRA and 2) to compare their performance, using GD-cMRA as the standard of reference (SOR).Methods
Twenty-two healthy subjects (10:12 M:F; 33±11.8 years; 72±15 kg) without contraindications to contrast-enhanced MRA were included in this prospective IRB-approved HIPAA-compliant feasibility study. Subjects underwent two visits, separated by ≥4 weeks. MRA was performed on a 3T clinical MR system (Discovery MR 750, GE Healthcare, Waukesha, WI) using a 32-channel torso coil (Neocoil, Pewaukee, WI). MR-acquisition parameters are summarized in Table 1.
Visit 1: GD-enhanced conventional- vs. UTE-MRA: Pulmonary MRA was started with a conventional multi-phase 3D T1-weighted breath-held spoiled gradient echo (SGRE) MRA with Cartesian k-space sampling before, during and after the injection of 0.1 mmol/kg GD diluted with saline to 30 ml. Subsequently, free-breathing GD-UTE-MRA was acquired as a series of three different flip angles (FA: 6°, 12°, 18°) to optimize T1 weighting. The order of the FA was changed randomly between subjects to either ascending or descending.
Visit 2: FE-enhanced conventional- vs. UTE-MRA: Subjects received 4mg/kg FE diluted with saline to 60 ml as a slow infusion over 15 minutes. Pulmonary MRA was started during the steady state of FE with a conventional 3D T1-weighted breath-held SGRE-MRA as a series of four different FA (6°, 12°, 18°, 24°) in a fixed order. Subsequently, free-breathing FE-UTE-MRA was acquired as a series of four different FA (6°, 12°, 18°, 24°) in a fixed order.
To determine the optimal FA for best relative T1 contrast between vasculature and PE, regions of interest (ROIs) were drawn into the left and right main and lower lobe pulmonary arteries, as well as paraspinal muscle which served as a reference tissue5. A linear mixed-effects model was used to test which FA resulted in highest signal intensity and highest relative contrast between vessel lumen and muscle.
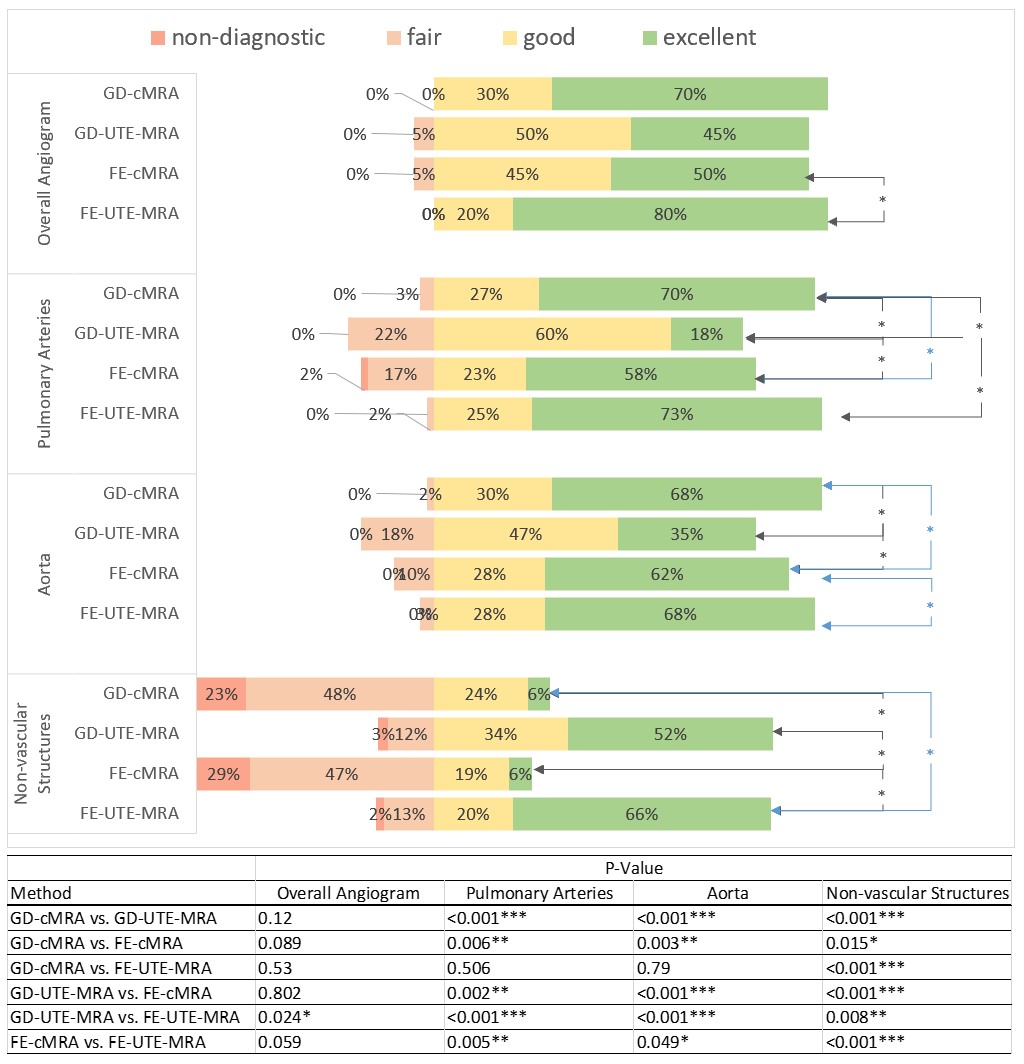
Two radiologists performed a direct side-by-side comparison consensus reading to assess subjective image quality of the three investigational MRA techniques (GD-UTE-MRA, FE-UTE-MRA, FE-cMRA) at their previously determined best FA, using multi-phase GD-cMRA as SOR. The image quality of vascular and non-vascular (lung, pleura, bronchi, esophagus, mediastinum, bone, soft tissue) structures was also rated on a 4-point Likert scale (0=nondiagnostic, 3=excellent). The Wilcoxon Sign-Rank Test was used to compare Likert-scale results between methods. Two-sided p-values < 0.05 were regarded as statistically significant.
Results
Two subjects did not participate in Visit 2 and were excluded from the study which therefore consisted of 20 subjects.
Representative image examples are shown in Figure 1 and 2. Best relative contrast between the pulmonary arteries and reference muscle was achieved at an FA of 18° for GD-UTE-MRA, 18° or 24° for FE-UTE-MRA and 24° for FE-UTE-MRA, respectively (p<0.05).
Results from image quality ratings are summarized in Figure 3. Overall image quality of the pulmonary angiogram was good or excellent for all four techniques and without any significant differences between FE-UTE-MRA and GD-cMRA (SOR). GD-UTE-MRA showed the lowest image quality of the angiogram due to low image contrast. Both UTE-MRA techniques showed significantly better image quality for the depiction of non-vascular structures than cMRA (Figure 3).
Discussion
This study investigated three alternative approaches for pulmonary MRA aiming to mitigate limitations of cMRA using gadolinium-based contrast agents. Our results suggest that free-breathing FE-UTE-MRA offers excellent image quality of the pulmonary vasculature while simultaneously allowing superior depiction of non-vascular structures compared to gadolinium enhanced breath-held Cartesian MRA. FE-UTE-MRA acquisition at high FA resulted in best contrast between vasculature and muscle (reference tissue for PE). Previous animal studies also demonstrated high diagnostic yield of FE-UTE-MRA for PE6. Further investigations are needed to determine the utility of this new approach in clinical practice.Conclusion
Free-breathing UTE-MRA using ferumoxytol is feasible for the evaluation of PE. The ultra-short echo times combined with radial sampling could help mitigate motion-related artifacts and allow simultaneous assessment of non-vascular structures. Larger patient studies should investigate the clinical utility of free-breathing UTE-MRA for assessment of PE.Acknowledgements
The authors wish to acknowledge support from the Departments of Radiology and Medical Physics, University of Wisconsin, as well as the NIH (T32CA009206 and K24 DK102595). Further, the authors wish to acknowledge GE Healthcare and Bracco diagnostics who provide research support to UW-Madison.
Gesine Knobloch and Tilman Schubert contributed to this work while employed by UW-Madison. G.K. is now an employee of Bayer AG, Berlin, Germany. T.S. is now an employee of the Department of Radiology, University Hospital Bern, Switzerland.
References
1. Francois CJ, Hartung MP, Reeder SB, Nagle SK, Schiebler ML. MRI for acute chest pain: current state of the art. Journal of magnetic resonance imaging : JMRI 2013;37(6):1290-1300.
2. Schiebler ML, Nagle SK, Francois CJ, Repplinger MD, Hamedani AG, Vigen KK, Yarlagadda R, Grist TM, Reeder SB. Effectiveness of MR angiography for the primary diagnosis of acute pulmonary embolism: clinical outcomes at 3 months and 1 year. Journal of magnetic resonance imaging : JMRI 2013;38(4):914-925.
3. Stein PD, Chenevert TL, Fowler SE, Goodman LR, Gottschalk A, Hales CA, Hull RD, Jablonski KA, Leeper KV, Jr., Naidich DP, Sak DJ, Sostman HD, Tapson VF, Weg JG, Woodard PK. Gadolinium-enhanced magnetic resonance angiography for pulmonary embolism: a multicenter prospective study (PIOPED III). Annals of internal medicine 2010;152(7):434-443, w142-433.
4. Knobloch G, Colgan T, Wiens CN, Wang X, Schubert T, Hernando D, Sharma SD, Reeder SB. Relaxivity of Ferumoxytol at 1.5 T and 3.0 T. Invest Radiol 2018;53(5):257-263.
5. Frydrychowicz A, Nagle SK, D'Souza SL, Vigen KK, Reeder SB. Optimized high-resolution contrast-enhanced hepatobiliary imaging at 3 tesla: a cross-over comparison of gadobenate dimeglumine and gadoxetic acid. Journal of magnetic resonance imaging : JMRI 2011;34(3):585-594.
6. Bannas P, Bell LC, Johnson KM, Schiebler ML, Francois CJ, Motosugi U, Consigny D, Reeder SB, Nagle SK. Pulmonary Embolism Detection with Three-dimensional Ultrashort Echo Time MR Imaging: Experimental Study in Canines. Radiology 2016;278(2):413-421.
Figures
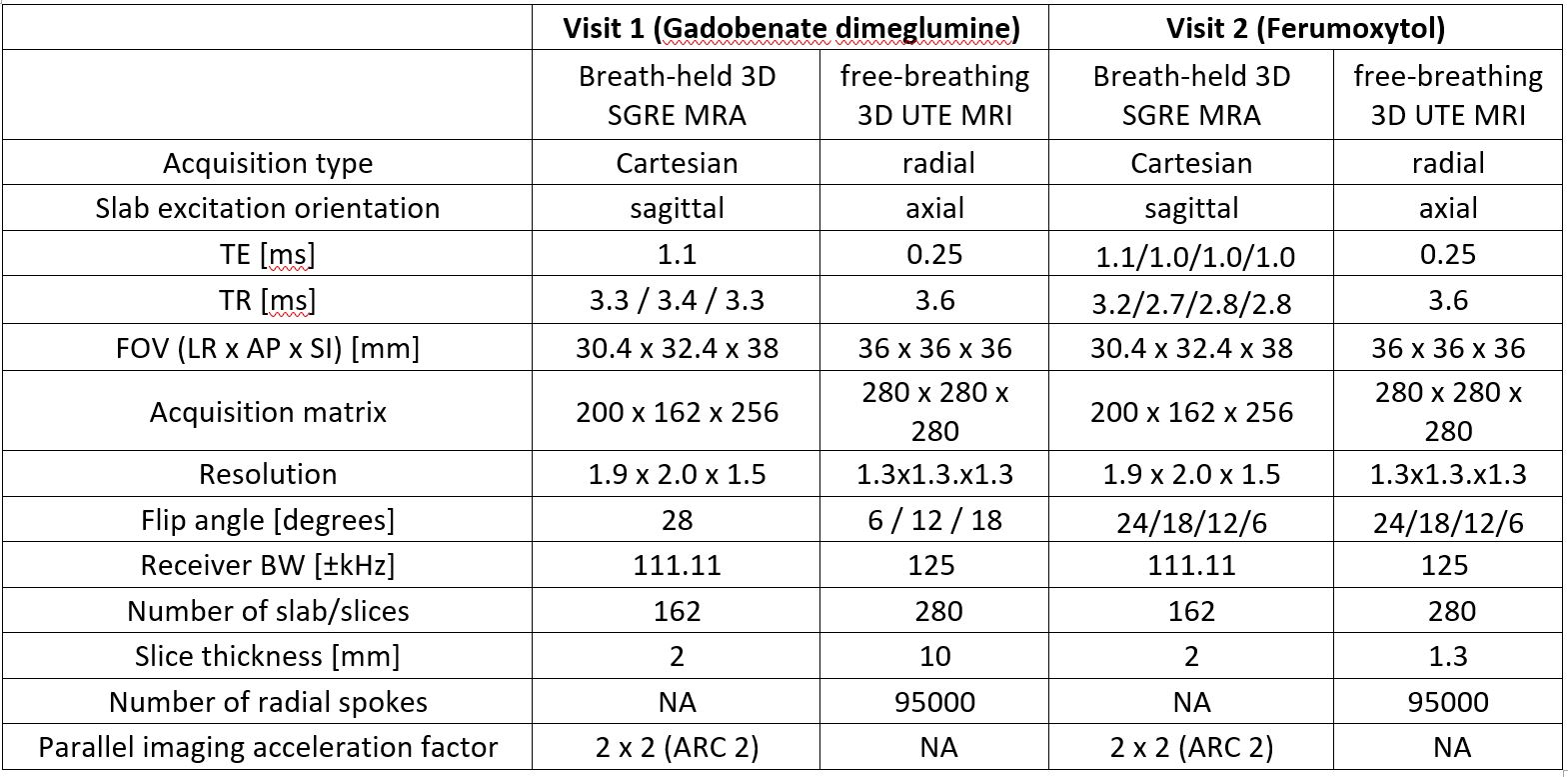
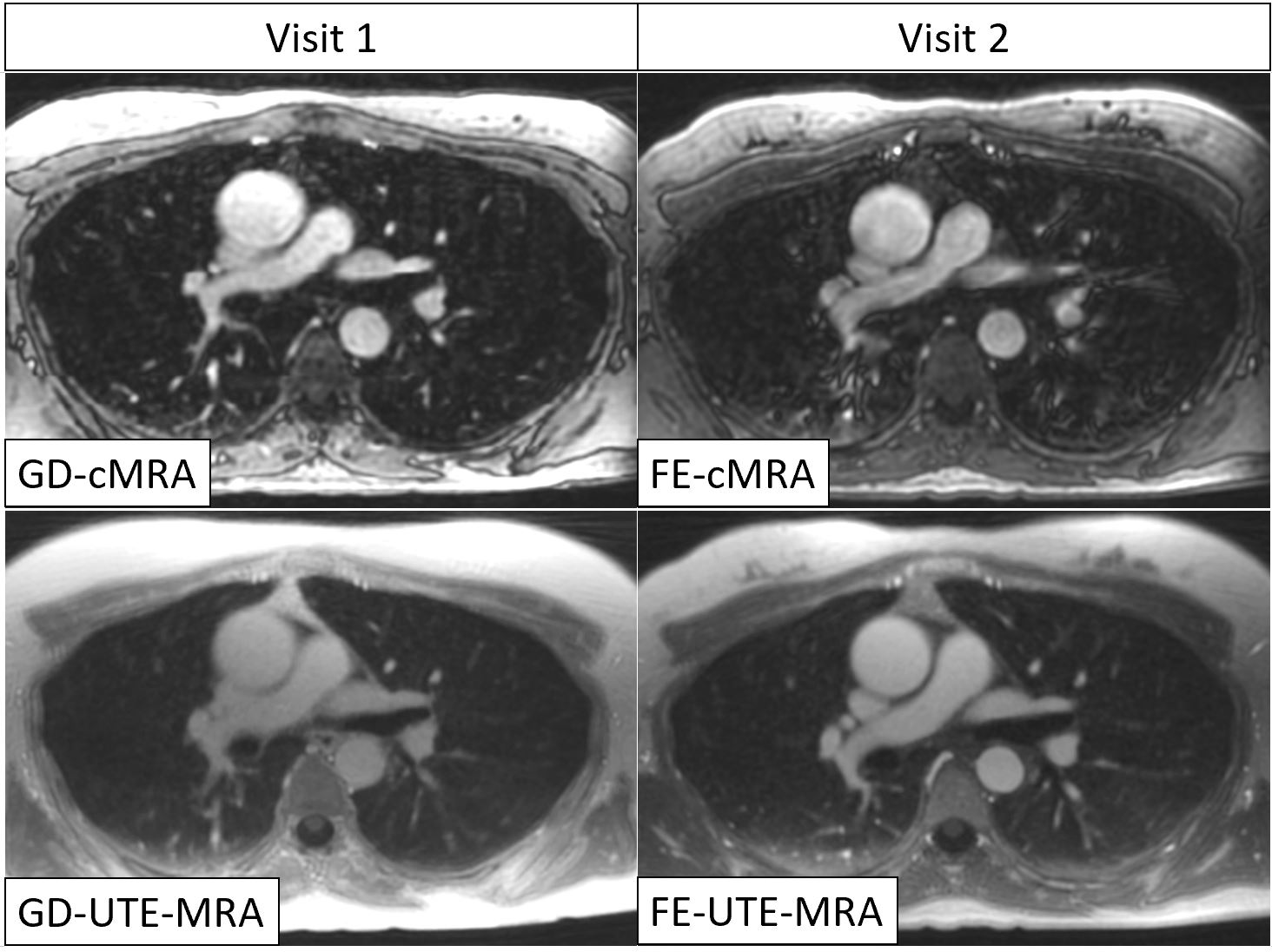
Figure 1: Representative image example of one subject at the height of the pulmonary truncus. Both UTE-MRA techniques (lower row) show superior depiction of non-vascular structures (lung, bone, bronchi, muscle) compared to conventional MRA using a gadolinium-based contrast agent (top left). Furthermore, FE-UTE-MRA also showed excellent image quality of the angiogram, comparable to GD-cMRA. GD-UTE-MRA suffers from low image contrast. Vascular structures appeared blurry in FE-cMRA.
GD-cMRA: gadobenate dimeglumine enhanced conventional MRA, FE-cMRA: ferumoxytol enhanced conventional MRA, GD-UTE-MRA: gadobenate dimeglumine enhanced ultra-short echo time MRA, FE-UTE-MRA: ferumoxytol enhanced ultra-short echo time MRA.
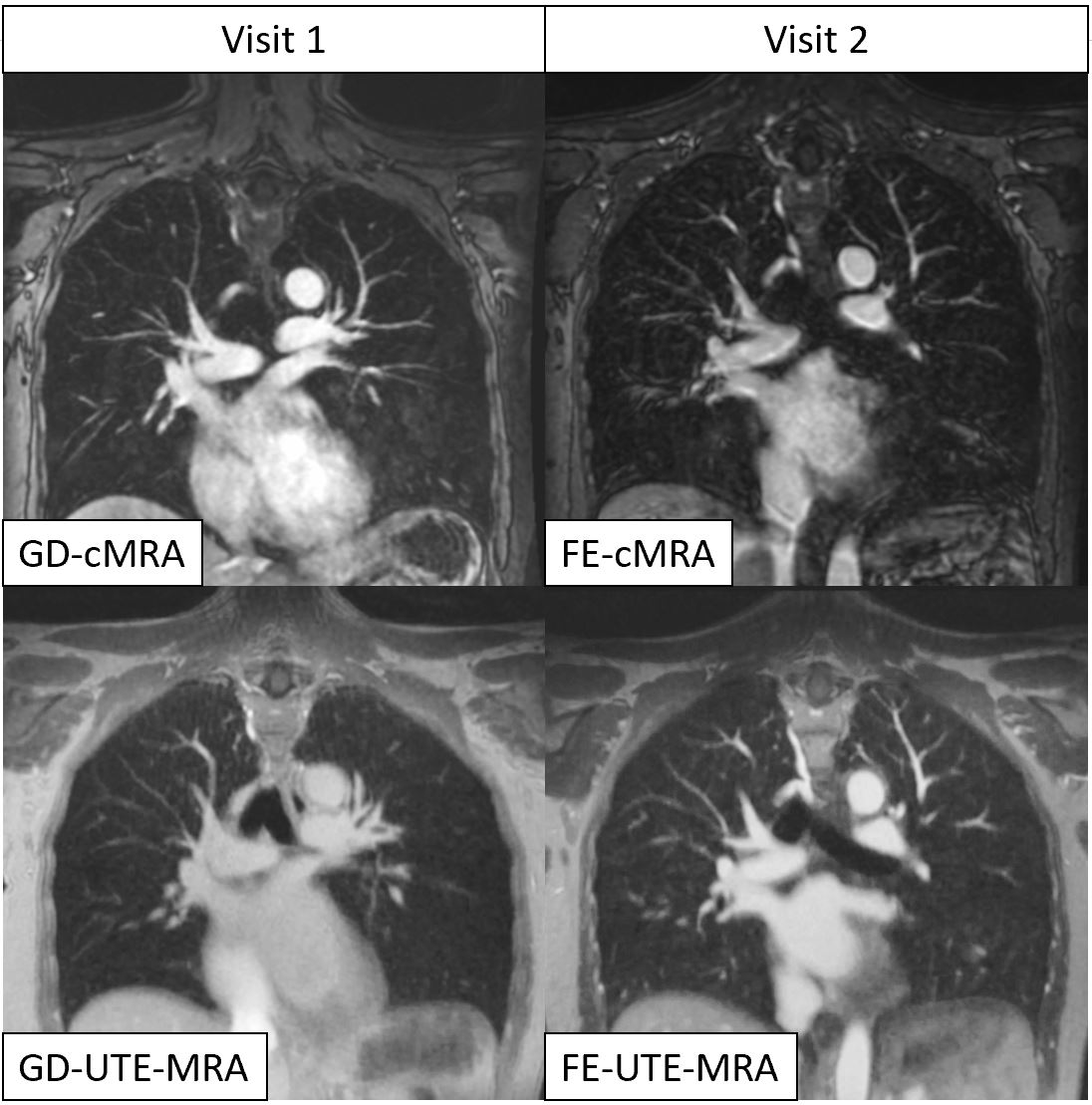
Figure 2: Coronal images through the thorax and mediastinum from one subject. Both UTE-MRA techniques (lower row) show superior depiction of non-vascular structures (lung, bone, bronchi, muscle) compared to conventional MRA using a gadolinium-based contrast agent (top left) or ferumoxytol (top right). FE-UTE-MRA also showed excellent image quality of the angiogram, comparable to GD-cMRA. GD-UTE-MRA suffers from low image contrast.
GD-cMRA: gadobenate dimeglumine enhanced conventional MRA, FE-cMRA: ferumoxytol enhanced conventional MRA, GD-UTE-MRA: gadobenate dimeglumine enhanced ultra-short echo time MRA, FE-UTE-MRA: ferumoxytol enhanced ultra-short echo time MRA.