2053
Free-breathing whole-heart coronary MRA with Radial SSFP and fully automated 3D rigid body motion corrected reconstruction1MR Clinical Science, Philips Healthcare, Best, Netherlands, 2Department of Biomedical Engineering, Eindhoven University of Technology, Eindhoven, Netherlands, 3MR R&D, Philips Healthcare, Bangalore, India
Synopsis
Prolonged acquisition time and susceptibility to respiratory motion remain to be the major challenge in 3D free-breathing whole-heart MR angiography. Recently, respiratory self-navigated 3D-Radial CMRA technique has been proposed to address the said limitations. In this technique, a 1-D projection oriented in Superior-Inferior direction are acquired at every heartbeat before each interleave of 3D-Radial imaging data for 1D motion correction of the heart with 100% respiratory gating efficiency. In this work, an extension of this method is proposed to estimate and correct for the 3D motion of the heart along with a robust navigator processing and automatic coil selection algorithm (3D-PRONAV). The proposed method is validated in five volunteers.
Introduction
Prolonged acquisition time and susceptibility to respiratory motion remain to be the major challenge in 3D free-breathing whole-heart (WH) MR angiography (CMRA). Cartesian acquisition in combination with respiratory gating and tracking is still the most widely used technique [1]. The relatively small acceptance window and the requirement of careful planning of the Navigator beam limit its applicability in clinical practice. Recently, respiratory self-navigated 3D-Radial CMRA technique has been proposed to address the above-mentioned limitations [2]. In this technique, a 1-D projection oriented in Superior-Inferior (SI) direction is acquired at every heartbeat before each segment of 3D-Radial data acquisition and is used for estimation of the rigid-body motion of the heart, allowing motion correction with100% respiratory gating efficiency. However, this method does not account for the motion of the heart in Anterior-Posterior (AP) and Right-Left (RL) directions which can lead to a local blurring of images [3]. In this work, an extension of this method is proposed to estimate the 3D motion of the heart with a robust navigator processing and automatic coil selection algorithm (3D-PRONAV). The proposed method is validated in five volunteers.Methods
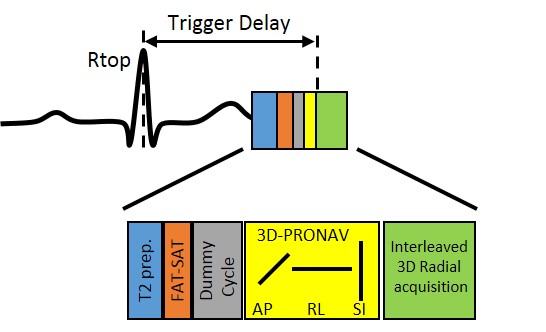
The proposed acquisition scheme is based on a balanced-SSFP sequence with 3D-Radial trajectory based on Spiral Phyllotaxis [4] modified to support anisotropic field-of-views (FOV) in XY and Z directions [5]. Three orthogonal projections were acquired in AP, RL and SI orientations (3D-PRONAV) respectively before each segment of image acquisition to derive motion information. The sequence is shown in figure 1. The algorithm proposed in this work to derive motion information from the 3D-PRONAV has the following steps,
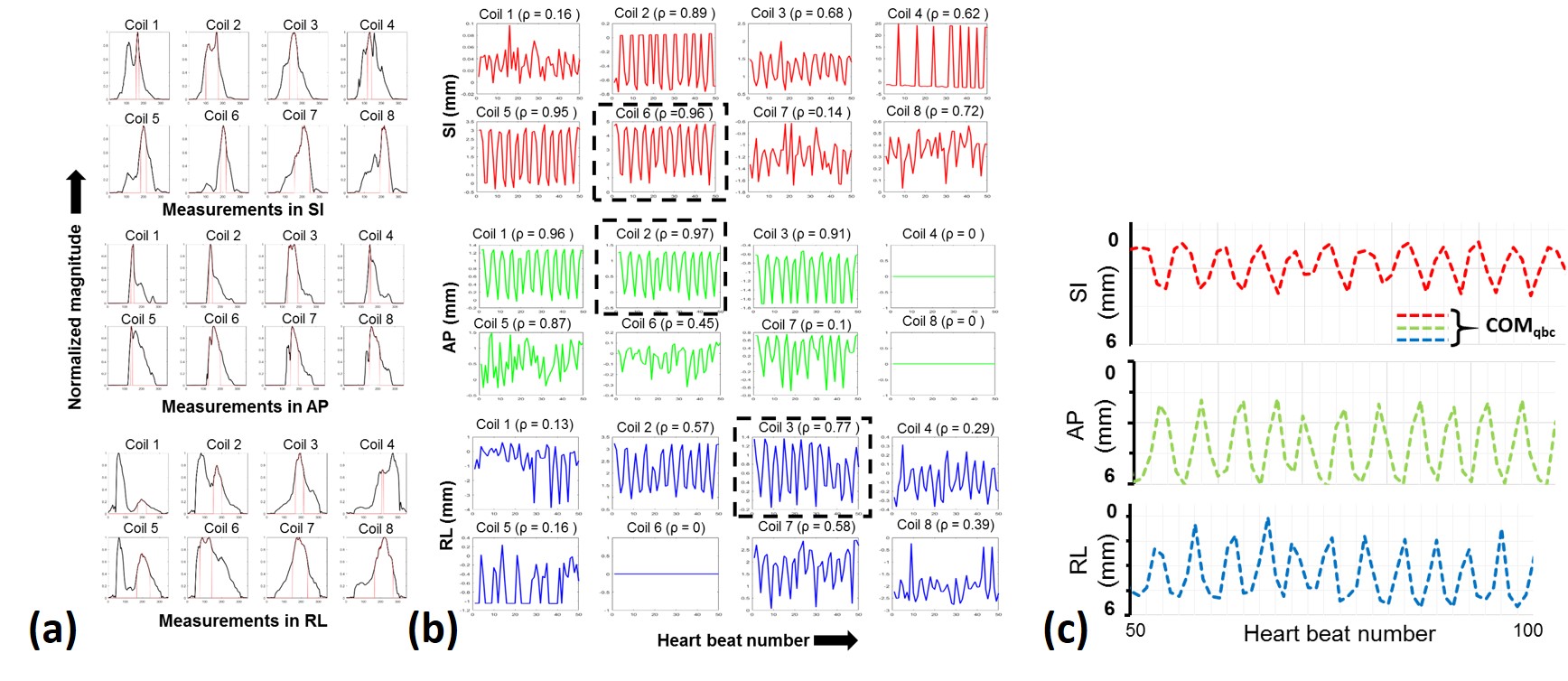
1. Segmentation of the blood pool (described in [2]) in the reference projection followed by cross-correlation to estimate motion with sub-mm precision from each anterior coil elements, mi - the motion estimate from coil i with i = 1,2.. N coil elements.
2. Computing motion based on center-of-mass in the quadrature body coil (COMqbc ) [6].
3. Selecting a coil which has the maximum correlation coefficient (ρmax), where ρmax = max(|ρ(COMqbc, mi )|), i Є {1,2,..N}, and ρ(COMqbc, mi) is the correlation coefficient (range from -1 to 1) between COMqbc and mi.
These steps were repeated for all the three projections to estimate the 3D rigid-body motion of the heart. 3D motion correction is performed in k-space prior to gridding according to the Fourier shift theorem. The proposed technique is implemented in a 1.5T Ingenia scanner (Philips Healthcare, Best, Netherlands). Five healthy volunteers were imaged for free-breathing WH CMRA. The images were analyzed using Soap-Bubble tool [7]. A pencil beam navigator motion data was additionally acquired for data analysis. The imaging parameters were; TE/TR: 1.7 / 3.7 ms, acquired aliasing-free FOV: ~ 117 X 117 X 58 mm, reconstructed FOV: (220 mm)3, resolution: (1.2 mm)3, flip angle: 90⁰, receiver bandwidth: 867 Hz/Pixels, volume selective with an FWHM of 220 mm in SI direction was used, 2 saturation slabs were positioned to suppress signals from right and left shoulders respectively, a total of 9048 to 12064 radial projections were acquired depending on the volunteer’s heart rate in 377 interleaves. The scan time for the proposed technique was in the range of 4.5 to 7.2 mins depending on the volunteer’s heart rate. Reconstructions were performed on the scanner immediately after acquisition with the reconstruction times of approx. 30sec.
Results
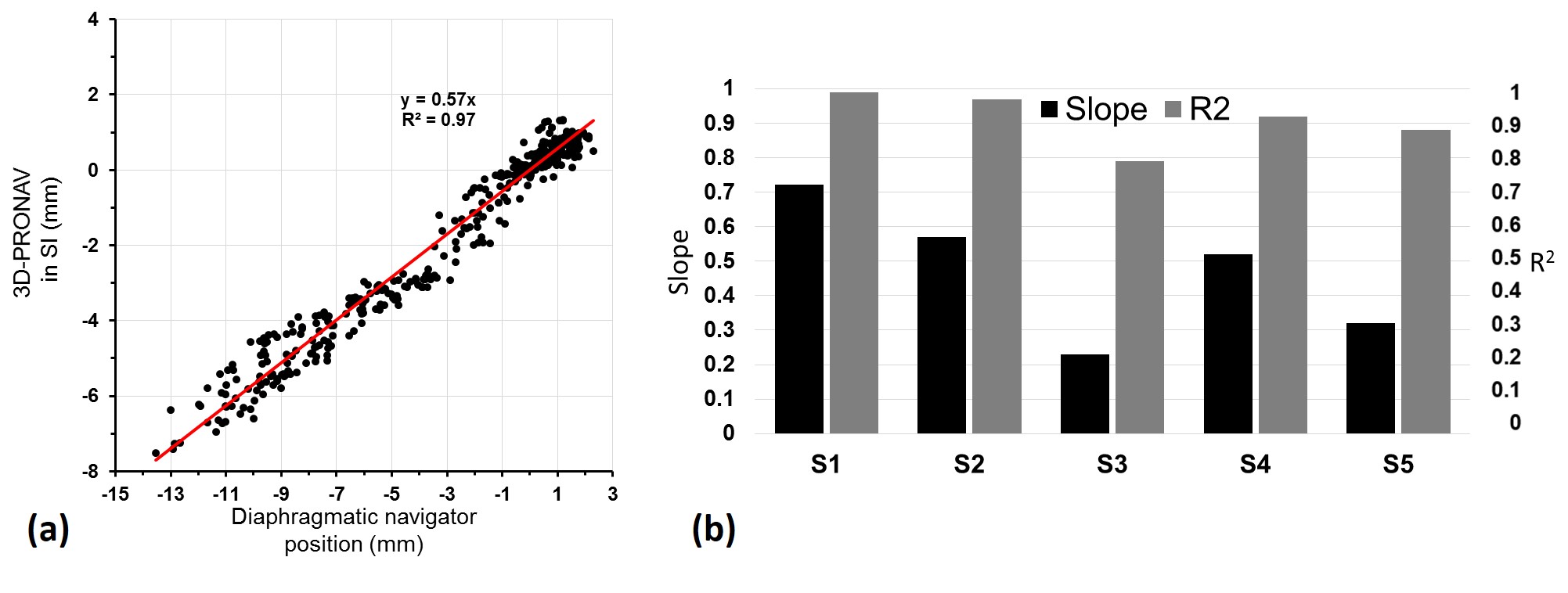
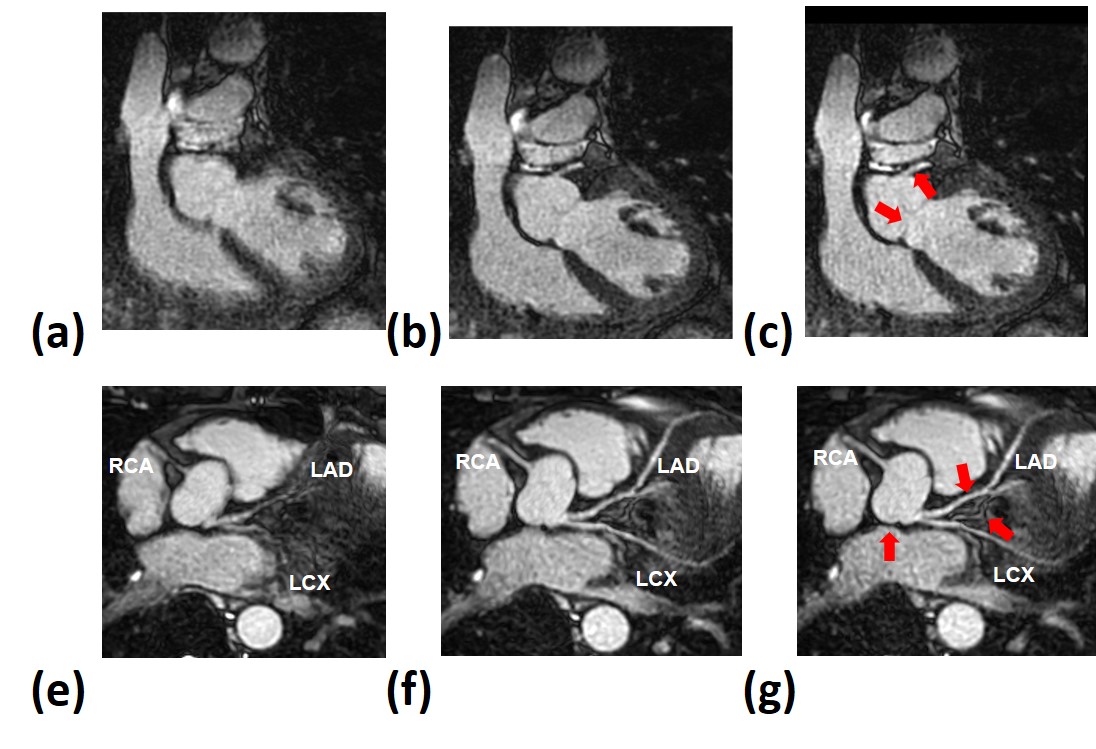
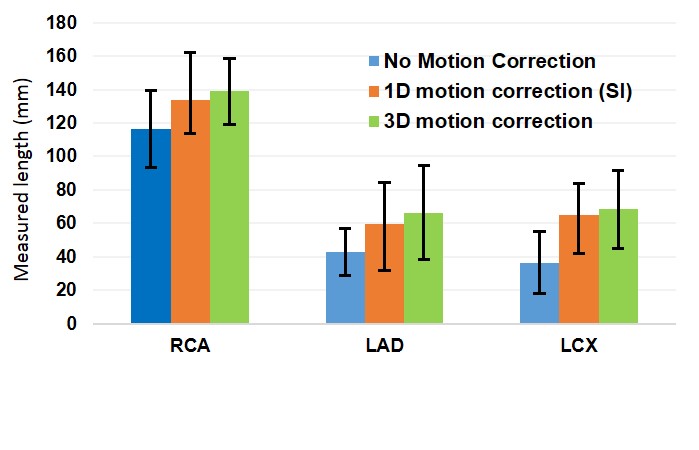
An example of the proposed motion estimation from the 3D PRO-NAV is shown in figure 2. Blood-pool segmentation in reference projections of 3D-PRONAV is shown in 2(a) and the estimated motion are shown in 2(b). The COMqbc is plotted in 2(b) and selected coils in 2(b) are highlighted. Comparison between the motion derived in SI from 3D-PRONAV and the pencil beam navigator is shown in Figure 3. Free-breathing WH CMRA images obtained from one of the volunteers using the proposed technique are shown in figure 4. The measured length of major coronary branches in five volunteers is shown in figure 5.Discussion and Conclusion
A new fully automatic method to estimate 3D translation motion of the heart from projection navigators (3D-PRONAV) has been proposed and validated. Motion correction in 3D resulted in better visualization of coronary arteries and overall sharper cardiac images compared to motion correction performed only in SI orientation for scans with 100% respiratory gating efficiencyAcknowledgements
This work was supported by the European Commission within the Horizon 2020 Framework through the MSCA-ITN-ETN European Training Networks (project number 642458).References
1. Stuber, M., et al., Submillimeter Three-dimensional Coronary MR Angiography with Real-time Navigator Correction: Comparison of Navigator Locations. Radiology, 1999. 212(2): p. 579-587.
2. Piccini, D., et al., Respiratory self-navigation for whole-heart bright-blood coronary MRI: Methods for robust isolation and automatic segmentation of the blood pool. Magnetic Resonance in Medicine, 2012. 68(2): p. 571-579.
3. Lai, P., et al., A respiratory self-gating technique with 3D-translation compensation for free-breathing whole-heart coronary MRA. Magnetic Resonance in Medicine, 2009. 62(3): p. 731-738. 4. Piccini, D., et al., Spiral phyllotaxis: The natural way to construct a 3D radial trajectory in MRI. Magnetic Resonance in Medicine, 2011. 66(4): p. 1049-1056.
5. Krishnamoorthy, G., Smink, J., Kouwenhoven, M., Breeuwer, M, Anisotropic Field-of-Views in 3D Golden Angle Radial Imaging. Proc. Intl. Soc. Magn. Reson. Med. 2018, 2018. 4130.
6. Stehning, C., et al., Free-breathing whole-heart coronary MRA with 3D radial SSFP and self-navigated image reconstruction. Magnetic Resonance in Medicine, 2005. 54(2): p. 476-480.
7. Etienne, A., et al., “Soap‐Bubble” visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magnetic Resonance in Medicine, 2002. 48(4 DOI - 10.1002/mrm.10253): p. 658-65866.
Figures