2052
Evaluation of quiescent-interval single-shot (QISS) magnetic resonance angiography (MRA) in diabetic patients with clinical limb ischemia in comparison with contrast-enhanced MRA with calf-compression at 3 Tesla1Shanghai Jiaotong University affiliated Sixth People's Hospital, Shanghai, China, 2MR Collaboration, Siemens Healthcare Ltd., Shanghai, China, Shanghai, China
Synopsis
Early diagnosis and aggressive management are critical to mitigate the devastating natural history of Critical limb ischemia (CLI). Computed tomography angiography (CTA) and contrast-enhanced magnetic resonance angiography (CE-MRA) are established methods in the diagnostic workup of PAD. However, the high incidence of infrapopliteal disease in CLI and the calcified nature of these vessels in patients suffering from diabetes mellitus are problems even for the dual-energy CT. In addition, diabetic patients with CLI frequently experience several comorbidities, which can hamper administration of iodinated contrast media and lead to contrast-induced nephropathy. What’s more, the high prevalence of chronic renal impairment in diabetic patients with CLI and CE-MRA studies often place such patients at an increased risk of nephrogenic systemic fibrosis. Quiescent-interval single-shot (QISS)-MRA is a robust non-enhanced MRA method that has shown promising results at 1.5 T and 3 T. Here, we wished to evaluate the image quality and diagnostic accuracy of QISS-MRA at 3 T in diabetic patients with CLI compared with CE-MRA with calf compression, with digital subtraction angiography (DSA) serving as the standard reference.
Introduction
Early diagnosis and aggressive management of critical limb ischemia (CLI) are critical to mitigate this condition’s devastating natural history. Computed tomography angiography (CTA) and contrast-enhanced magnetic resonance angiography (CE-MRA) are established methods for diagnosing peripheral arterial disease. However, calcified infrapopliteal vessels, which are commonly found in diabetic patients suffering from peripheral arterial disease, are not imaged well on CT and even on dual-energy CT. In addition, diabetic patients with CLI frequently experience renal dysfunction, which can prohibit administration of both iodinated and gadolinium contrasts. Quiescent-interval single-shot (QISS)-MRA is a robust non-enhanced MRA method that has shown promising results on 1.5T and 3T scanners. In this study, we aim ed to evaluate the image quality and diagnostic accuracy of QISS-MRA at 3T in diabetic patients with CLI and to compare it with CE-MRA with calf compression.method
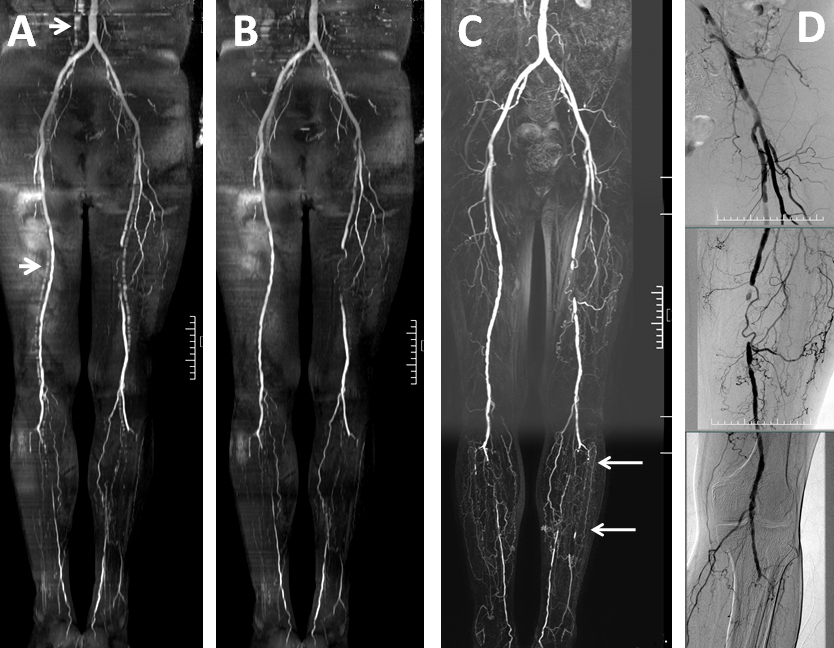
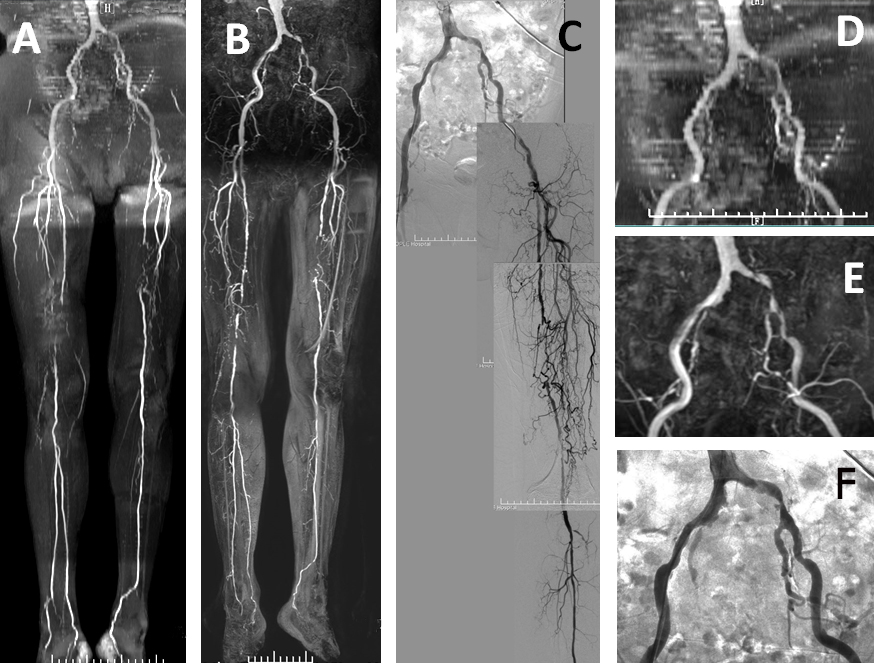
Thirty-seven diabetic patients with CLI underwent QISS-MRA, CE-MRA, and DSA, the last of which served as the standard of reference. QISS-MRA was undertaken on a 3T system (MAGNETOM Verio, Siemens Healthcare, Erlangen, Germany) using a combination of superficial body array matrix coils for the abdomen and pelvis, a 36-element peripheral angiography matrix coil, and a large 4-channel flex coil (Fig. 1-2). A prototype QISS sequence was applied. The phase of magnetization preparation was followed by a quiescent interval of 226 ms, during which no excitation took place. The following imaging parameters were used: field of view, 400 × 266 mm2; axial plane; 2D; matrix, 400 × 260; measured voxel size, 1.0 × 1.0 × 3.0 mm3; reconstructed voxel size, 0.5 × 0.5 × 3 mm3; repetition time, 813 ms; echo time, 1.45 ms; flip angles per slab of 60°; generalized autocalibrating partially parallel acquisitions (GRAPPA) with an acceleration factor of 2; partial Fourier acquisition in the phase-encoding direction, 5/8. To span the entire arterial system from the pelvis to the feet, we acquired eight groups of 70 slices with a slice thickness of 3.0 mm and an overlap of 0.6 mm. Image quality (five-point Likert scale) and stenosis severity (five-point grading scale) for QISS-MRA and CE-MRA were evaluated by two blinded readers. DSA results served as the reference for stenosis severity. Per-segment and per-region sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated.results
Image quality of QISS-MRA and CE-MRA in all 1147 segments was evaluated. Stenosis severity was assessed on QISS-MRA and CE-MRA and was analyzed in 654 vessel segments. Image quality of QISS-MRA was lower compared with CE-MRA in the pelvic region (p<0.001 in both reader 1 and reader 2) and thigh region (p=0.033 in reader 1 and p = 0.018 in reader 2), whereas in the calf region, the image quality of QISS-MRA was better than CE-MRA (p=0.009 in reader 1 and p=0.001 in reader 2). In segment-based and region-based analyses, there was no difference between QISS-MRA and CE-MRA in sensitivity (89.5% vs. 90.3%, p=0.774 in reader 1 and 87.6% vs, 90.6%, p=0.266 in reader 2) and specificity (94.2% vs. 92.9%, p=0.513 in reader 1 and 92.9% vs. 92.9%, p=1.000 in reader 2). Region-based analyses also showed that QISS-MRA and CE-MRA yielded similar sensitivity and specificity values in all regions except the pelvis where a difference in specificity was observed (95.5% vs. 84.8%, p=0.041).discussion
In the present study, QISS-MRA generated good-quality images in diabetic patients with CLI. The image quality of QISS-MRA was comparable with that of CE-MRA, and was particularly good in the distal thigh and calf. Using DSA as the reference standard, the diagnostic accuracy of QISS-MRA was high. In QISS-MRA, a pre-saturation pulse is used inferior to the slice to suppress the signal from venous blood. However, venous overlap was found frequently in pelvic and calf stations upon study commencement. We attempted to adjust the venous pre-saturation slab thickness for pelvic (100mm), thigh and calf stations (40mm), which resulted in remarkable venous suppression. Meanwhile, the venous contamination was eliminated at calf station on QISS-MRA. Another challenge of QISS-MRA in diabetic patients with CLI is motion artifact. QISS-MRA has a longer scan time than CE-MRA, so the tendency for diabetic patients with CLI to move their legs caused by pain at rest can result in degradation of image quality.conclusion
QISS-MRA performed very well in diabetic patients with CLI and may be a good alternative for patients with contraindications to CE-MRA. QISS may be particularly useful for the diagnosis of diabetic peripheral vascular disease which preferentially involves arteries below the knee with lower-limb ulceration or other risk factors.Acknowledgements
No acknowledgement found.References
No reference found.Figures