2042
Hyperpolarized Magnetic Resonance Reveals Cardiac and Hepatic Metabolic Dysfunction in the ZDF Model of Type 2 Diabetes1Department of Physiology, Anatomy and Genetics, University of Oxford, Oxford, United Kingdom, 2Department of Physics, University of Oxford, Oxford, United Kingdom, 3Oxford Centre for Clinical Cardiac Magnetic Resonance Research, University of Oxford, Oxford, United Kingdom, 4Cardio Metabolic Research, University of Leeds, Leeds, United Kingdom, 5Novo Nordisk, Måløv, Denmark
Synopsis
The Zucker Diabetic Fatty (ZDF) rat is a well-known hyperinsulinaemic and hyperlipidaemic model of severe uncompensated Type 2 diabetes (T2DM) that displays systolic cardiac dysfunction late in life at the 40 week timepoint. Hyperpolarized Magnetic Resonance (MR) is a new medical imaging technique that can provide a novel way to probe metabolism in vivo and has been widely used to demonstrate physiological and pathological changes in pyruvate metabolism in the rodent heart. This work presents a magnetic resonance characterisation of the ZDF rat with hyperpolarized MR that detects metabolic alterations prior to the development of cardiac dysfunction.
Purpose
Cardiovascular complications represent the leading cause of diabetes-related morbidity and mortality in the developed world.[1–4] Recent work has shown that drugs that improve cardiovascular outcomes in diabetes, such as metformin and the SGLT2 inhibitor Empagliflozin alter the metabolic phenotype of the diabetic heart by altering either redox state[5] or the rate of ketone body utilisation respectively.[6] In this work, we examined the cardiac and hepatic metabolic phenotype of a severe model of T2DM, the Zucker Diabtic Fatty (ZDF) rat, with the aim of both quantifying metabolic impairment and providing a platform for future interventional studies.Methods
12 week old ZDF rats and littermate lean controls ($$$n=4$$$ per group) given Purina 5008 ad libitum were anaesthetised (isoflurane in $$$\text{O}_2,\,2\,\text{l}\,\text{min}^{-1}$$$) fortnightly and subjected to cardiovascular and hepatic multiparametric MRI to obtain cardiac volumes and ejection fractions, myocardial fat/water content via PRESS $$$^1$$$H spectroscopy, metabolic information via dual-slice selective hyperpolarised $$$^{13}$$$C spectroscopy following [1-$$$^\text{13}$$$C]pyruvate infusion, and hepatic T$$$_{1}$$$/T$$$_{2}^{*}$$$ relaxometry maps via Look-Locker inversion recovery or multi-echo imaging. Rats were scanned at baseline (12 weeks old), two weeks and four weeks into the study, based on previous descriptions of the development of diabetes in these animals.
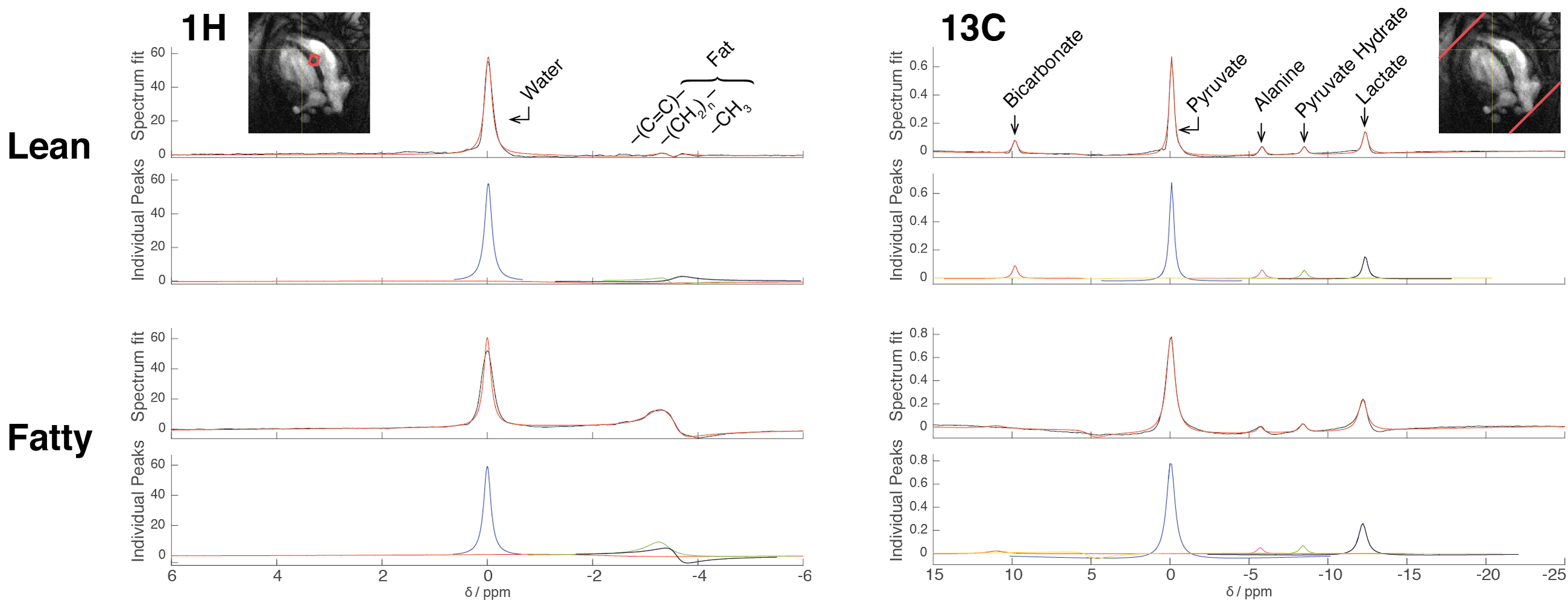
Briefly, cardiac volumes were obtained by prospectively gated FLASH CINE ($$$51.2\times51.2\times1.6\,\text{mm}^3$$$ FOV, $$$192\times192$$$ matrix, 10 slices, 50 frames, 150 kHz bandwidth); PRESS 1H spectroscopy with 60 averages from a $$$2\,\text{mm}^3$$$ voxel placed in the mid ventricular septum; $$$2\,\text{s}$$$ TR; $$$10\,\text{ms}$$$ TE; $$$4\,\text{kHz}$$$ bandwidth. Hepatic Look-Locker T1 maps were acquired with a $$$5^\circ$$$ FA, 8 TIs between $$$0.1\,\text{s}$$$ and $$$4\,\text{s}$$$, $$$128\times128$$$ matrix, $$$51.2\times51.2\times2\,\text{mm}^3$$$ FOV. T$$$_{2}^{*}$$$ maps were obtained by multi-echo gradient echo images at the same resolution. Hyperpolarised spectra were obtained by slice-selective spectroscopy from both the heart and liver following tail vein infusion of $$$2\,\text{ml}$$$ [1-$$$^\text{13}$$$C]pyruvate hyperpolarised at 3.35T/1.4K ($$$10\,\text{mm}$$$ thick slab, $$$15^\circ$$$ FA, 8 kHz bandwidth). All imaging was performed in the fed state early in the morning.
Food intake and body weight were determined daily. Fed glucose and ketone concentrations were determined at the same time as scanning via a hand-held meter, and rats were subject to an IV glucose tolerance test following an overnight fast at baseline or after six weeks. All statistical analyses were performed via either GrowthCurveR or blme4 in R.
Results
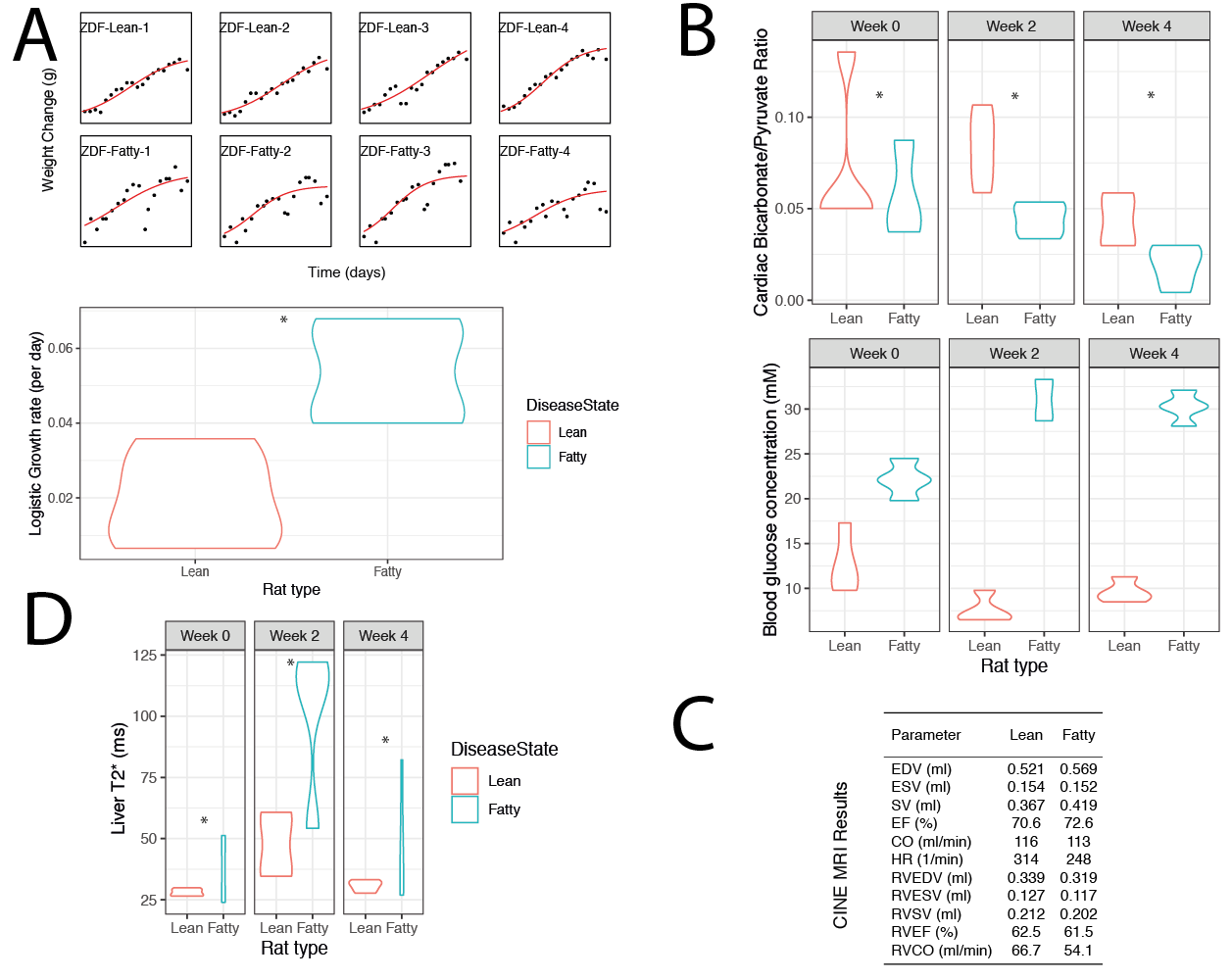
The ZDF Rat maintains a highly obese, diabetic phenotype at 12--16 weeks of age, with no distinct cardiac phenotype at this timepoint, although it is reported that diastolic dysfunction does develop by 40 weeks of age.[7] Hyperpolarised carbon or proton spectral data obtained from the myocardium was of good quality (Fig. 1). We confirmed that the ZDF phenotype is hyperglycaemic ($$$p<10^{-16}$$$) and obese (growth curve analysis $$$p<0.05$$$); c.f. Fig. 2A,B.
Hyperpolarized spectroscopy detected a cardiac ($$$p=0.001$$$) and hepatic ($$$p=0.01$$$) reduction in PDH flux (c.f. Fig. 2B) that became significantly increased over time ($$$p=0.01$$$). Cardiac and hepatic lactate production was not changed. Myocardial proton spectroscopy did not indicate a statistically significant increase in myocardial triglycerides, but it was observed that myocardial lipid accumulation was highly variable between animals. At this timepoint, no cardiac dysfunction was observed (C).
Likewise, relaxometry measurements indicated a significant ($$$p=0.03$$$) increase in hepatic T$$$_{2}^{*}$$$ in the ZDF rat, consistent with the reported development of non-alcoholic fatty liver disease and the associated fibrosis. Hepatic T1 was not significantly altered.
Discussion
Despite lifelong hyperglycaemia and metabolic alterations, the ZDF rat possesses a relatively minor cardiac phenotype when compared to other rodent models of T2DM and indeed obesity and CV-risk-factor adjusted patient populations. Our work has shown that, at these time points, there is little evidence of global myocardial fat deposition despite profound metabolic alterations, weight gain, and hyperglycaemia. However, it is known that at later timepoints the ZDF rat decompensates and succumbs to systolic cardiac dysfunction and severe hepatic and myocardial steatosis. The only significant alteration to the ZDF heart during the studied period is the increasing and profound reduction in PDH flux as detected via hyperpolarised pyruvate MRS that we believe is consistent with the hypothesis that metabolic alterations drive functional decline in the diabetic heart.Conclusion and Future Work
Our work shows that hyperpolarized magnetic resonance is a sensitive and powerful predictor of future cardiac dysfunction at a timepoint where few other methods can detect pathology. Future work will aim to further understand the cardiovascular physiology of the ZDF rat, and explore novel biology in ameliorating its diabetic phenotype.Acknowledgements
JJM is supported by a Novo Nordisk Postdoctoral Fellowship run in partnership with the University of Oxford. All authors would like to acknowledge the British Heart Foundation, the NHS NIHR, and EPSRC.References
[1] S. Boudina, E. D. Abel, Diabetic cardiomyopathy revisited, 2007.
[2] M. Marjańska, I. Iltis, A. A. Shestov, D. K. Deelchand, C. Nelson, K. Uğurbil, P.-G. G. Henry, K. Uurbil,P.-G. G. Henry, K. Uğurbil, P.-G. G. Henry, K. Uurbil, P.-G. G. Henry, K. Uğurbil, P.-G. G. Henry, J. Magn. Reson. 2010, 206, 210–218.
[3] D. J. Tyler, Curr. Cardiovasc. Imaging Rep. 2011, 4, 108–115.
[4] M. Mishkovsky, A. Comment, R. Gruetter, J. Cereb. Blood Flow Metab. 2012, 32, 2108–2113.
[5] A. J. Lewis, J. J. Miller, C. McCallum, O. J. Rider, S. Neubauer, L. C. Heather, D. J. Tyler, Diabetes2016, 18, db160804.
[6] D. Abdurrachim, X. Q. Teo, C. C. Woo, W. X. Chan, J. Lalic, C. S. P. Lam, P. T. H. Lee, Diabetes Obes.Metab. 2018, DOI 10.1111/dom.13536.
[7] A. Daniels, D. Linz, M. Van Bilsen, H. Rütten, T. Sadowski, S. Ruf, H. P. Juretschke, C. Neumann-Haefelin, C. Munts, G. J. Van Der Vusse, F. A. Van Nieuwenhoven, Eur. J. Heart Fail. 2012
Figures