2039
A Magnetization Recovery Matched TI-Scout for Exact Determination of Inversion Time in Segmented Inversion Recovery Gradient Echo Imaging for Late Gadolinium Enhancement1Siemens Healthineers, Durham, NC, United States, 2Duke Cardiovascular MR Center, Duke University, Durham, NC, United States
Synopsis
We present a new TI-scout sequence based on multiple single-shot GRE acquisitions with timing and readout parameters matched to segmented inversion recovery imaging for which optimal TI is to be determined. Temporal magnetic evolution of the scout is identical to that of the segmented GRE sequence for LGE. The new technique substantially improves upon the existing SSFP cine-based TI scout that typically underestimates TI and provides mediocre image quality. We show accurate TI determination by comparison with gold standard TI found by an expert and compare image quality and signal ratios of existing, new TI scout, and segmented LGE.
INTRODUCTION
In late Gadolinium Enhancement (LGE), finding the optimal inversion time (TI) is crucial for maximum infarct-to-myocardium contrast. This requires repeating the breath-held LGE sequence to iteratively find optimal TI, which is time-consuming for expert technologists and difficult for beginners. Existing cine-based TI-scouts [1] (CBTIS) can help, but typically provide suboptimal TI estimates and require a long breath-hold. They use steady state free precession (SSFP) readout (RO) spanning the entire cardiac cycle, whereas LGE uses segmented gradient echo (GRE) RO occupying only a fraction. These differences in RO type and duration result in different magnetic saturation and thus a poor TI estimate by CBTIS. Furthermore CBTIS image quality (IQ) is frequently poor as magnetization never reaches the full steady state common in cine SSFP. Lastly, existing CBTIS cannot be combined with magnetization- and timing-affecting features such as fat-inversion by Spectral Attenuated Inversion Recovery (SPAIR) and artifact post-suppression [2]. We therefore designed a new single-shot GRE TI-scout (NTIS) with timing and readout parameters identical to SEGLGE, for which TI is sought. Thereby temporal magnetic evolution of NTIS should be matched to SEGLGE and optimal TI precisely determined. We evaluated TI accuracy of NTIS and CBTIS by comparison to a gold standard TI (GSTI) determined by an expert technologist. We scored image quality (IQ) and calculated myocardium over blood contrast ratio (MBR) of NTIS, CBTIS, and SEGLGE. We compared IQ and MBR among these groups.
METHODS
On a 3T clinical MR scanner (MAGNETOM VIDA, Siemens Healthineers) an expert technologist acquired segmented breath-held LGE (SEGLGE) images after administration of a T1-shortening Gadolinium contrast agent (Gadoterate Meglumine) iteratively finding GSTI. Next, NTIS acquired 10 free-breathing single-shot images with different TI, followed by a breath-held CBTIS scan. NTIS and CBTIS acquired images at 10 identical TI values (240, 265,…, 465 ms). CBTIS acquired additional shorter and longer TI images throughout the cardiac cycle from TI[1] to TI[n] (25ms increments). Figure 1 shows all sequences. Magnetic saturation and recovery relevant parameters RO flip angle, echo spacing, lines per segment, and recovery beats were matched between SEGLGE and NTIS. Matching temporal resolution of segmented and single-shot RO was feasible by fourfold parallel acceleration and lower spatial resolution of NTIS. An experienced reader blinded to TI values selected the NTIS and CBTIS images with the optimal LGE contrast. Resulting TI values were compared to GSTI with a paired two-tailed t-test. In SEGLGE, NTIS and CBTIS, IQ was assessed on a four point scale and MBR was calculated as normal myocardium over blood signal. The same test compared NTIS and CBTIS with SEGLGE images, respectively, regarding IQ and MBR.RESULTS
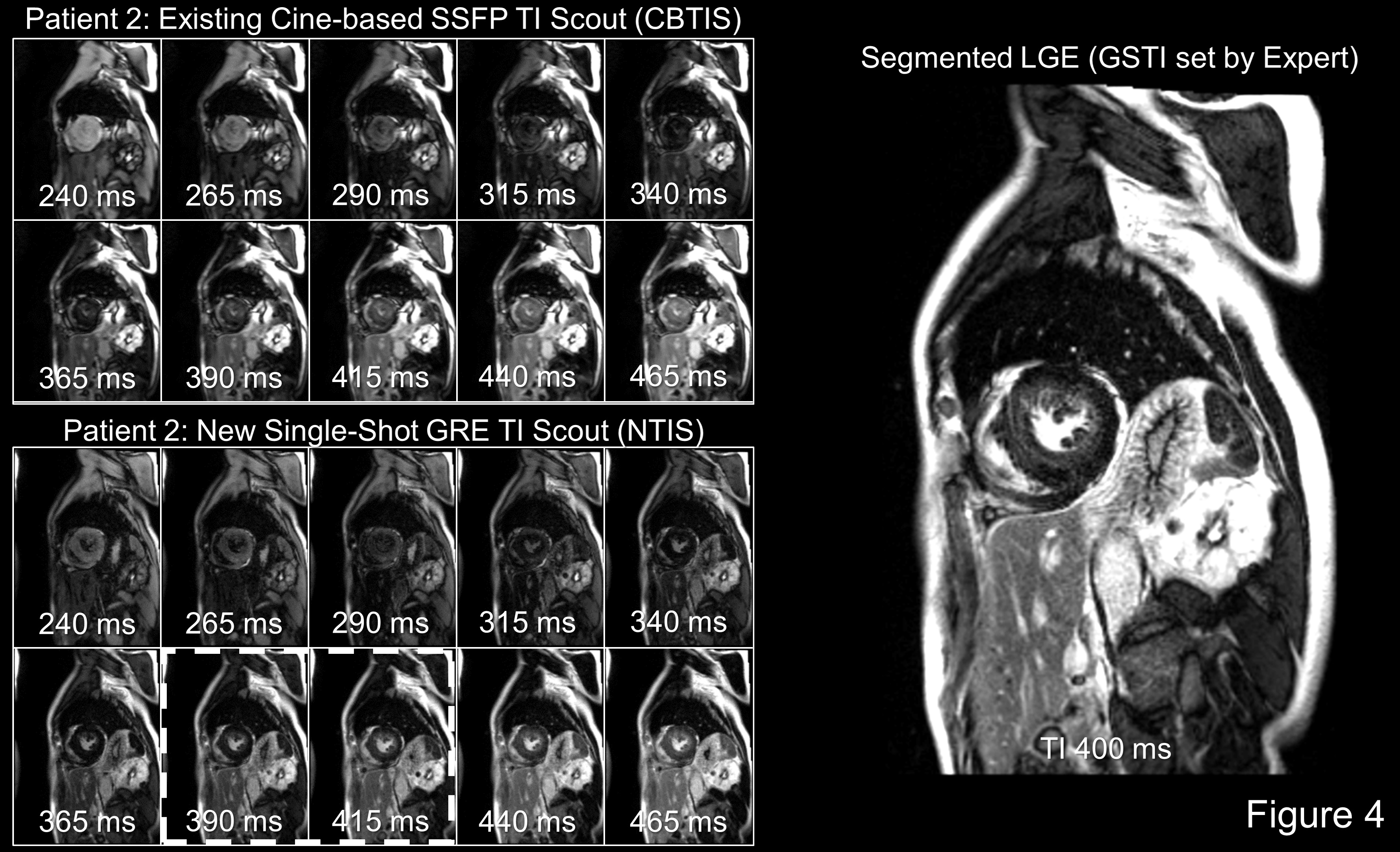
35 slices were acquired in 26 patients (11 F, 15 M, average RR 897±222ms). The CBTIS images with TI<240ms and TI>465ms were beyond useful TI range and discarded. The table (Figure 2) shows IQ, MBR, and the difference between optimal TI found by either scout and GSTI. Optimal TI was statistically identical to GSTI for NTIS, but significantly different (p<0.0001) for CBTIS, about 53 ms shorter. Figure 3 illustrates the common finding of TI underestimation by CBTIS. MBR was identical between NTIS and SEGLGE, but significantly lower for CBTIS compared to SEGLGE (p<0.05). CBTIS IQ was significantly worse than SEGLGE (p<0.0001), but identical between NTIS and SEGLGE. Figure 4 shows the occasional problem of CBTIS that optimal TI occurs during systole where substantially no blood pool is visible due to cardiac contraction, making determination of optimal image contrast challenging.
DISCUSSION
NTIS finds TI with anticipated accuracy, without the requirement of repeated breath-holds. Picking optimal TI from NTIS images is much easier than from CBTIS images, since image contrast of NTIS and SEGLGE is identical for the same TI, and all NTIS images come from the same diastolic phase. It is interesting that the reader perceived image contrast to be optimal in the CBTIS image which in fact had a smaller myocardium to blood contrast than the SEGLGE image. We attribute this finding to the difference in SSFP and GRE image appearance.
CONCLUSION
NTIS should facilitate accurate TI determination in LGE imaging for experienced and beginning technologists alike, thereby making image contrast optimal and consistent across patients. Magnetization evolution would be exactly matched between NTIS and SEGLGE also if other magnetization-affecting pulses and modules (SPAIR, post suppression) were activated for SEGLGE, as they would also be for NTIS. Since all NTIS images are at the same diastolic phase, automated TI determination from these images by motion correction and automatic cavity and myocardium detection may be feasible.Acknowledgements
References
[1] Amano Y, Takayama M, Kumita S. Contrast-enhanced myocardial T1-weighted scout (Look-Locker) imaging for the detection of myocardial damages in hypertrophic cardiomyopathy. J Magn Reson Imaging. 2009; 30(4):778–784.
[2] Jenista E, Rehwald W, Chaptini N, et al. Suppression of ghost artifacts arising from long T1 species in segmented inversion‐recovery imaging. Magn Reson Med 2016; 78:1442–1451.
Figures
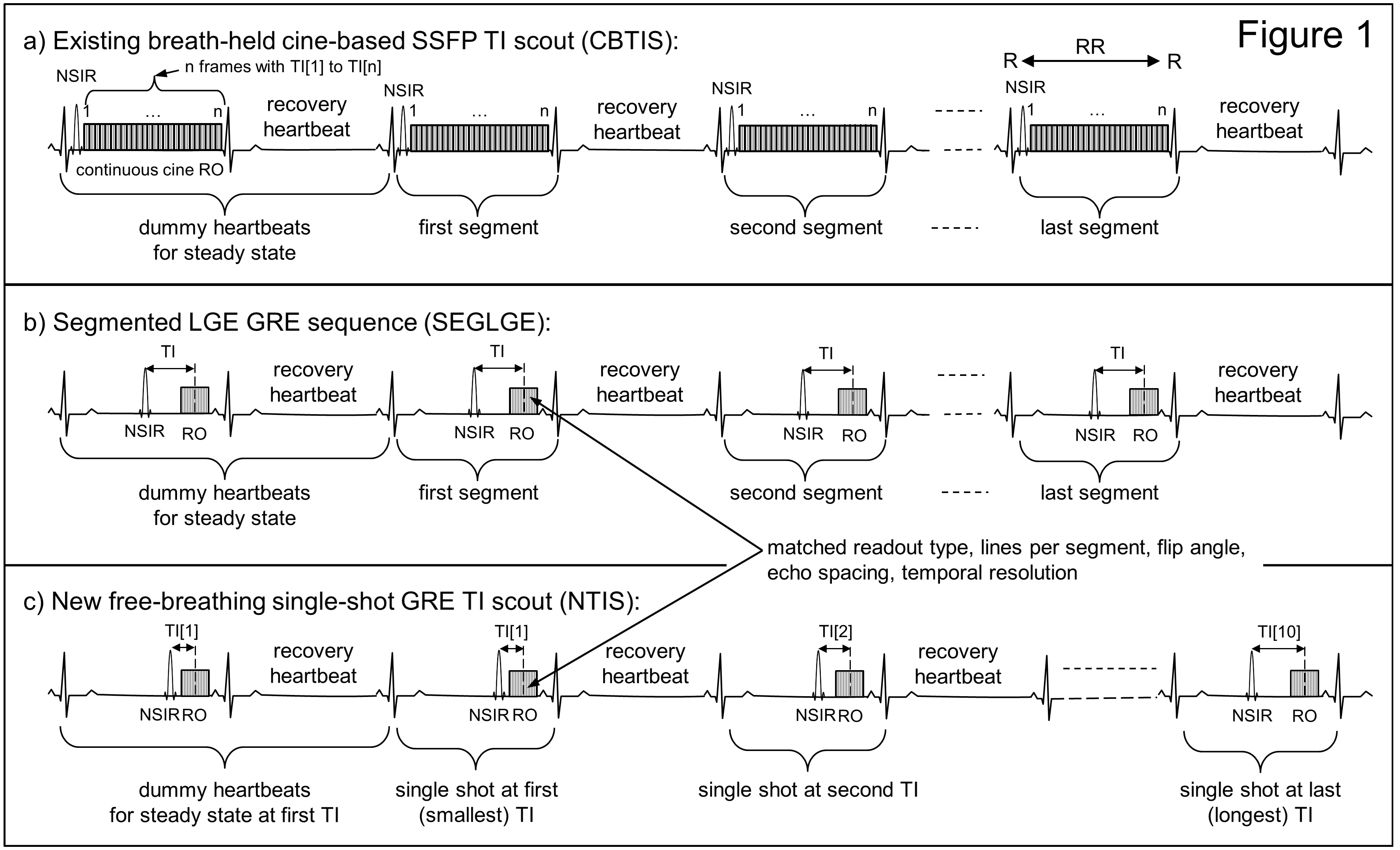
a) Sequence diagrams of CBTIS, b) SEGLGE, and c) NTIS. Acquisition and recovery beats interleaved. Parameters:
CBTIS: fov 360mmx81%, matrix 192x50%, partial Fourier 7/8, 1.9x1.9x8mm, flip 35°, TE 1.37ms, echo spacing 3.14ms, temporal resolution 25ms, bandwidth 840 Hz/pixel, segments 8, duration 20 RR breath-held.
SEGLGE: fov 360mmx81%, matrix 320x80%, 1.1x1.1x6mm, parallel acquis. (PAT) factor 2, 128 external reference lines, flip 19°, TE 2.37ms, echo spacing 5.32ms, temporal resolution 186ms, bandwidth 347Hz/pixel, segments 35, duration 8 RR breath-held.
NTIS parameters matched SEGLGE except fov 360mmx75%, matrix 192x97%, 1.9x1.9x8 mm, PAT factor 4, single shot, 10 measurements, duration 22 RR free-breathing.

Results of image quality (IQ) assessment, normal-myocadium to blood signal ratio measurements, and difference of scout-derived optimal TI to gold standard TI (GSTI). IQ, MBR, and optimal TI are identical between segmented LGE images and NTIS images, but different from respective values obtained in CBTIS images.

This patient example shows TI scout images of CBTIS on the top and NTIS on the bottom. The segmented LGE image on the right uses gold standard TI (GSTI) of 400ms determined by an expert operator. The TI scout images chosen by the blinded reader as having optimal image contrast are marked by a hatched white frame. Image 5 was chosen for CBTIS (TI = 340ms) and image 7 for NTIS (TI = 390ms), which was closer to the gold standard TI. CBTIS underestimated TI. Note the small subendocardial anterior wall infarct (arrow).
Another patient example shows the TI scout images of CBTIS on the top and NTIS on the bottom. The blinded reader picked NTIS images 7 and 8 as having optimal image contrast, see hatched white frame (TI 390ms - 425ms), which matches GSTI of 400ms used in the segmented LGE image on the right. Note that CBTIS images show the heart during systolic contraction. Therefore, hardly any blood pool is visible in the image at optimal TI and its vicinity, which is why selection of the optimal TI was cumbersome with CBTIS in this patient.