2037
Different Myocardial Perfusion Status in Acute Myocardial Infarction and Infarct-like Myocarditis: A Novel Intravoxel Incoherent Motion Diffusion-Weighted Imaging based MRI Study.1Renji Hospital Shanghai Jiao Tong University School of Medicine, Shanghai, China, 2Circle Cardiovascular Imaging, Calgary, AL, Canada
Synopsis
This study was to evaluate the diagnostic value of myocardial perfusion in patients with acute myocardial infarction (AMI) and “infarct-like myocarditis” using IVIM-DWI imaging. And the results showed: 1. Insufficient oxygen in the necrotic or infarted myocardium might affect myocardial perfusion and function. 2. IVIM-DWI may be a reliable sequence to evaluate different myocardial perfusion patterns in acute myocardial infarction and infarct-like myocarditis. 3. Acute myocardial infarction may exhibit lower myocardial perfusion status compared with infarct-like myocarditis due to different pathophysiological process.
Background
Acute myocarditis is common disease with 75% patients presenting with infarct-like manifestations of chest pain, raised troponin, but absence of obstructive coronary arteries 1-5. In this challenging clinical setting, it is requiring a series of clinical tests to identify acute myocarditis from myocardial infarction. In our prior study, we found that a dynamic process exists in the status of myocardial edema and myocardial perfusion in MI patients after PCI through the technique of intravoxel incoherent motion diffusion-weighted imaging (IVIM-DWI) 6. IVIM-DWI may provide more accurate information especially of microcirculation than conventional monoexponential model DWI 7,8.
We hypothesized that AMI patients would show more pejorative myocardial perfusion environment as well as reduced peak strain when compared with acute myocarditis patients and normal controls. The purpose of this study was to evaluate the diagnostic value of myocardial perfusion and altered mechanical parameters including IVIM-DWI imaging and tissue tracking in patients with acute myocardial infarction (AMI) and “infarct-like myocarditis”.
Method
CMR data from twenty patients with suspected AMI and twenty patients with “infarct-like myocarditis” (association of acute chest pain, elevated Troponin levels and ST-elevation) were retrospectively analyzed. Twenty age- and gender-matched healthy subjects served as control. IVIM-DWI data were acquired using multi-b valule single-shot spin-echo echo-planar imaging (SE-EPI) sequence. IVIM-DWI data were generated according to the 16-segments AHA-model and segmental values and pixel-standard deviation (SD) were recorded. Cine sequences covering left and right ventricle in short axis and three long axis were analyzed using a dedicated tissue tracking algorithm.Result
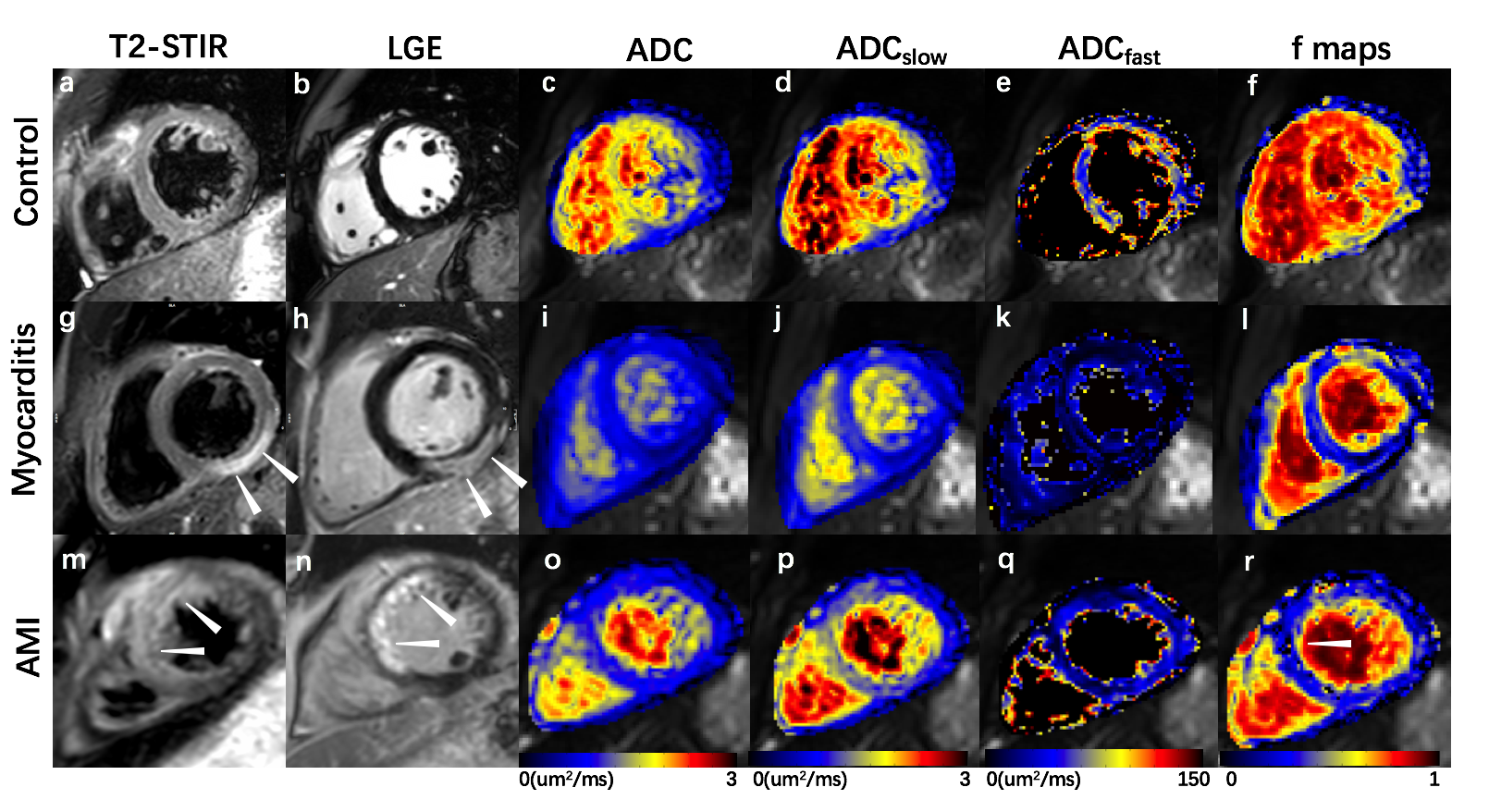
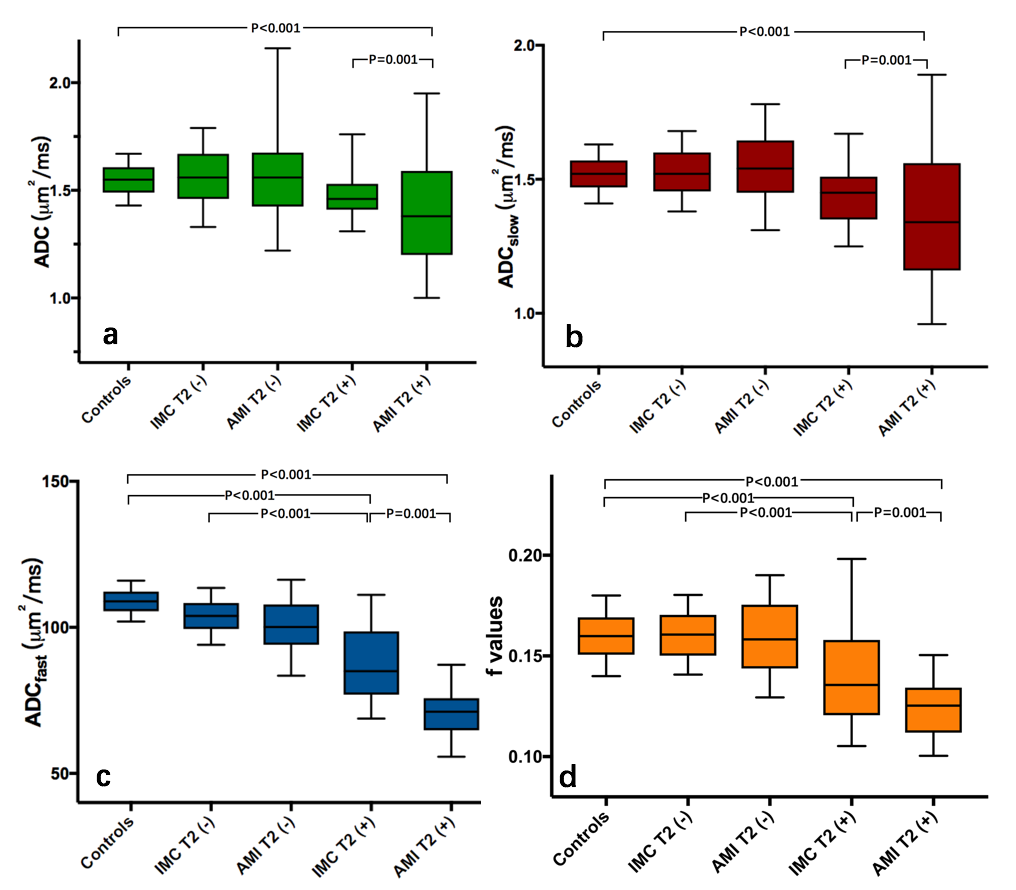
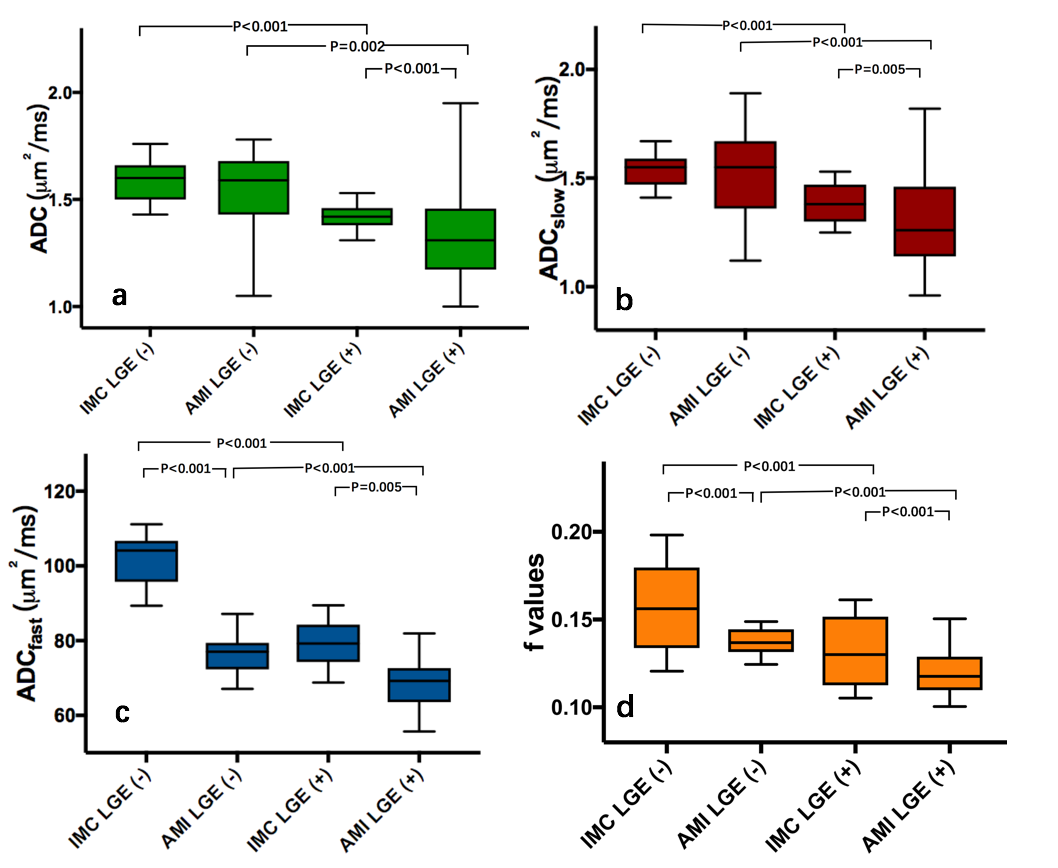
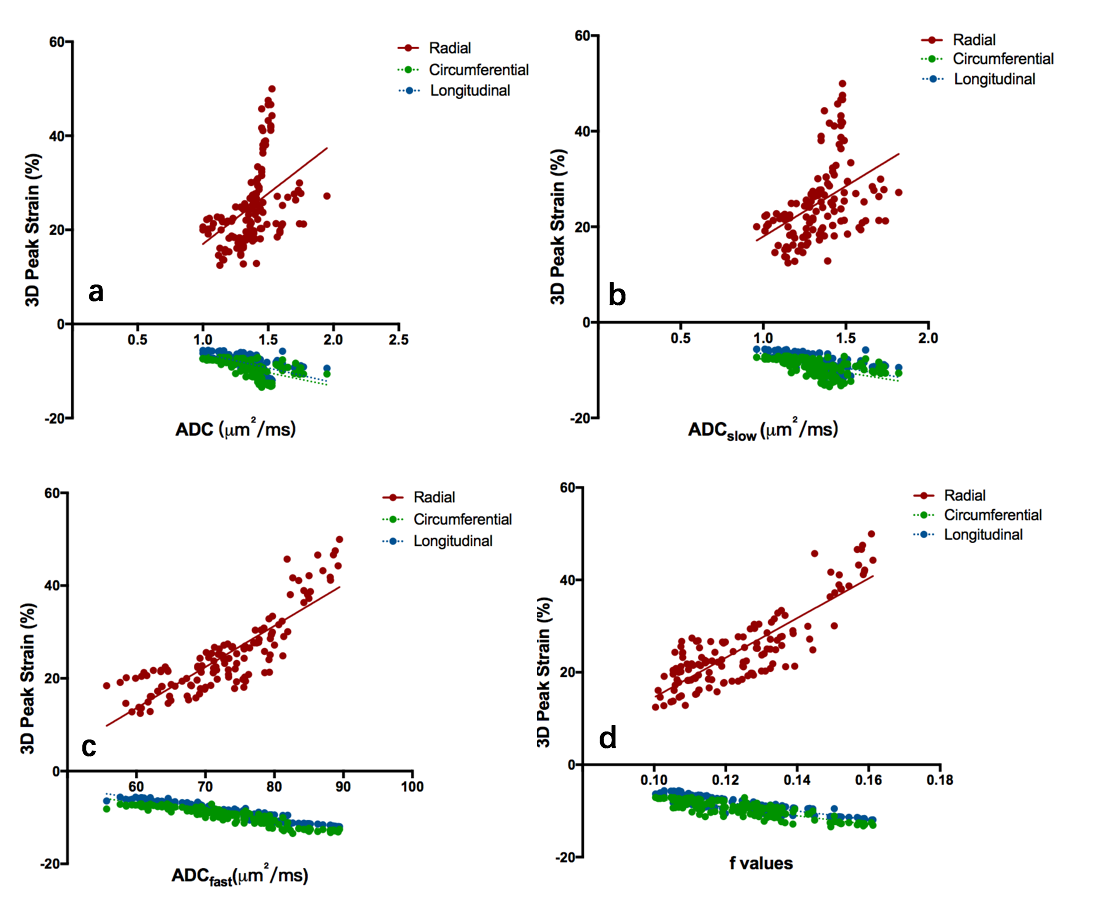
Overall, the AMI T2+ segments exhibited decreased ADC, ADCslow, ADC fast and f values (1.39±0.23μm2/ms, 1.36±0.23μm2/ms, 70.77±7.04μm2/ms and 0.1243±0.01) compared with infarct-like myocarditis T2+ (1.48±0.11μm2/ms, 1.44±0.11μm2/ms, 87.66±12.50μm2/ms and 0.1411±0.02) and normal controls(1.55±0.07μm2/ms, 1.52±0.06μm2/ms, 108.84±4.06μm2/ms and 0.1599±0.01) ( respectively, P<0.05), while AMI LGE+ segments showed lower IVIM-DWI associated parameters (1.34±0.21μm2/ms, 1.31±0.21μm2/ms, 68.75±6.33μm2/ms and 0.1198±0.01)than infarct-like myocarditis LGE+(1.42±0.06μm2/ms, 1.38±0.08μm2/ms, 79.12±5.70μm2/ms and 0.1313±0.02)(P<0.05). Left ventricular peak sub-endo and sub-epi radial strain, circumferential strain and longitudinal strain were lower in AMI T2+ segments than infarct-like myocarditis T2+ segments and normal controls (P<0.05), and AMI LGE+ segments exhibited the lowest strain on three orientations than other subgroups (P<0.05). Furthermore, IVIM-DWI associated parameters were linearly associated with myocardial strain in LGE+ groups.Discussion
In this study, IVIM-DWI demonstrated an excellent diagnostic performance in detecting different myocardial perfusion status in acute myocardial infarction and infarct-like myocarditis. Both in AMI and IMC groups, lower ADC, ADCslow, ADCfast and f values were detected in T2+ areas compared with T2- areas, and in LGE+ segments compared with LGE-T2+ segments. Lower IVIM values (including ADC, ADCslow, ADCfast and f values) were associated with lower radial, circumferential and longitudinal peak strain in LGE+ segments of both AMI and IMC groups which indicated severe myocardial injury.
Using the robust DWI-IVIM technique in the present study, we have demonstrated in patients of onsite myocardial infarction and myocarditis that IVIM associated parameters were significantly decreased in edematous( T2+ areas) and necrotic (LGE+ areas) myocardium compared to remote myocardium. In this result, edema caused by increased cellularity after myocardial injury accounted for the decreased ADC values due to the T2-weighting of the applied DWI-EPI sequence. Futher, impaired microvascular perfusion also contributed to the decreased ADC values in myocarditis or myocardial infarcted regions. Base on our knowledge, there may three reasons which could explain the reduced ADCfast or f values in myocardial infarction and myocarditis. First of all, microvasculature structure abnormalities in both myocardial infarction and myocarditis. Secondly, decreased capability of capillary to transport oxygen and metabolites in injured myocardium. Thirdly, reduced extracellular space volume fraction due to myocardial edema in tissue level. Interestingly, to the result of the current study, IVIM associated parameters decreased more in infarted myocardium than in myocarditis. This result presented that myocardial infartion may mainly cause vasogenic edema while myocarditis result in cytotoxic edema. Additionally,lower IVIM values were associated with lower radial, circumferential and longitudinal peak strain in LGE+ segments of both AMI and IMC groups which indicated severe myocardial injury. This result reflected that insufficient oxygen in the necrotic or infarted myocardium might impair myocardial funtion. Several studies have shown that tissue tracking enables reproducible assessment of myocardial strain accurately in myocardial infarction or myocarditis patients, and this method may provide prognostic information to a certain degree 9-11.
Conclusion
These findings prove IVIM-DWI may be a reliable sequence to evaluate different myocardial perfusion patterns in AMI and infarct-like myocarditis. AMI may exhibit lower myocardial perfusion status compared with infarct-like myocarditis due to different pathophysiological process.Acknowledgements
National Natural Science Foundation of China (No.81873887 and No.81873886) ; Shanghai Jiao Tong University medical cross project YG2017QN44; Shanghai Municipal Commission of Health and Family Planning excellent young talent program(No. 2017YQ031) ,References
1. Assomull RG, Lyne JC, Keenan N et al. The role of cardiovascular magnetic resonance in patients presenting with chest pain, raised troponin, and unobstructed coronary arteries. Eur Heart J 2017;28:1242-1249
2. Baccouche H, Mahrholdt H, Meinhardt G et al. Diagnostic synergy of non-invasive cardiovascular magnetic resonance and invasive endomyocardial biopsy in troponin-positive patients without coronary artery disease. Eur Heart J 2009;30:2869-2879.
3. Cooper LT, Jr. Myocarditis. N Engl J Med 2009;360:1526-1538
4. Gallagher S, Jones DA, Anand V et al. Diagnosis and management of patients with acute cardiac symptoms, troponin elevation and culprit-free angiograms. Heart 2012;98:974-981
5. Monney PA, Sekhri N, Burchell T et al. Acute myocarditis presenting as acute coronary syndrome: role of early cardiac magnetic resonance in its diagnosis. Heart 2011;97:1312-1318
6. An DA, Chen BH, Rui W et al. Diagnostic performance of intravoxel incoherent motion diffusion-weighted imaging in the assessment of the dynamic status of myocardial perfusion. J Magn Reson Imaging. DOI: 10.1002/jmri.26179. [Epub ahead of print]
7. Callot V, Bennett E, Decking UK et al. In vivo study of microcirculation in canine myocardium using the IVIM method. Magn Reson Med 2003;50:531-540
8. Mou A, Zhang C, Li M, Jin F et al. Evaluation of myocardial microcirculation using intravoxel incoherent motion imaging. J Magn Reson Imaging 2017;46:1818-1828
9. Luetkens JA, Schlesinger-Irsch U, Kuetting DL et al. Feature-tracking myocardial strain analysis in acute myocarditis: diagnostic value and association with myocardial oedema. Eur Radiol 2017;27:4661-4671
10. Nucifora G, Gillebert C, Selvanayagam JB. Value of novel cardiac magnetic resonance indices for the diagnosis of acute myocarditis: Left ventricular mechanics and parametric mapping imaging. International Journal of Cardiology 2016;223:881-882
11. Yoon YE, Kang SH, Choi HM et al. Prediction of infarct size and adverse cardiac outcomes by tissue tracking-cardiac magnetic resonance imaging in ST-segment elevation myocardial infarction. Eur Radiol 2018;28:3454-3463
Figures