2035
Rapid cardiac diffusion-weighted imaging with novel motion-compensated spherical tensor encoding1Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds, Leeds, United Kingdom, 2Clinical Sciences, Lund University, Lund, Sweden, 3Harvard Medical School, Boston, MA, United States, 4Brigham and Women's Hospital, Boston, MA, United States, 5Division of Cardiovascular Medicine, Radcliffe Department of Medicine, University of Oxford, Oxford, United Kingdom
Synopsis
Cardiac diffusion-weighted imaging (CDWI) is an emerging method for non-invasive assessment of cardiac microstructure. In CDWI, averaging and triggering are routinely used to mitigate motion artefacts, which results in long acquisition times. We have developed a novel motion-compensated spherical tensor encoding technique that reduces the acquisition time by a factor of up to three. Quantitatively, the method yields similar mean diffusivity as conventional methods, but enables accurate measurements in less than a minute.
Purpose
Cardiac diffusion-weighted imaging (CDWI) is an emerging contrast-free method for non-invasive assessment of cardiac microstructure. The diffusion of water in tissues is affected by a range of disease processes including inflammation, oedema, remodelling and scar formation, and the mean diffusivity (MD) can serve as a potential imaging biomarker. For example, an increase in MD is observed in myocardial infarction,1 hypertrophy,2 and dilated cardiomyopathy.3 Today, quantification of the MD requires measurements in at least 3 diffusion-encoding directions, because conventional diffusion-weighted imaging utilise so-called linear tensor encoding (LTE). This results in long scan times, which limit the feasibility of including CDWI in scanning of patient cohorts. Here we accelerate CDWI by using isotropic diffusion encoding, also known as spherical tensor encoding (STE).4,5,6 By developing a novel motion-compensated STE (mcSTE), CDWI was accelerated by a factor of 3 compared to LTE.Methods
Four sets of diffusion encoding gradient waveforms were implemented: LTE and STE without motion compensation (M0-LTE and M0-STE) and LTE and STE with 1st and 2nd order motion compensation (M2-LTE and M2-STE).Since asymmetric gradient waveforms were used to boost efficiency, we also took care to cancel effects of the concomitant gradients.7,8 Experiments were performed on a Prisma 3T MRI scanner (80mT/m @ 200 T/m/s) and body and spine RF coil arrays (Siemens Healthineers, Erlangen, Germany). Single-shot spin echo EPI data were acquired in a cylinder phantom filled with NiSO46H2O aligned along the Z-direction and subsequently in a double oblique manner simulating the position of the heart. A short axis stack was acquired at a simulated ECG of 60 beats per minute: TR = 3 RR-intervals, TE = 100 ms, ZOOM-IT, cardiac triggering, field-of-view = 320×111 mm2, resolution = 2.3×2.3 mm2, slices = 3, slice thickness = 8 mm, partial Fourier = 6/8, bandwidth = 2012 Hz/voxel, number of signal averages (NSA) = 8, blow = 100 s/mm2 and bhigh = 450 s/mm2, diffusion directions = 3 (X, Y, Z in LTE) / 1 (isotropic in STE), acquisition time = 2:24 min (LTE) / 0:48 min (STE) excluding scanner preparation time. Data are also reported for NSA = 1 (first of eight averages), where the acquisition time = 0:18 min (LTE) / 0:06 min (STE) excluding scanner preparation time. A non-zero low b-value was used to minimise the contribution of myocardial perfusion.9 The experiments were repeated in free-breathing healthy volunteers (N=6). Written consent was obtained from all volunteers. To correct for cardiac motion, volunteer data were affinely registered in Elastix.10 MD was calculated in Matlab (Mathworks, Natick, USA) in the phantom and volunteer data according to Equation 1, where E(b) is the normalised signal attenuation and N is the number of diffusion directions. The myocardium was manually segmented based on a mean diffusion-weighted (DW) image averaged across all b-values and DW directions.
\[MD = \frac{1}{N} \sum_i^N=\frac{-\log(E(b_{i}))}{b_{high}-b_{low}} [1]\]
Results
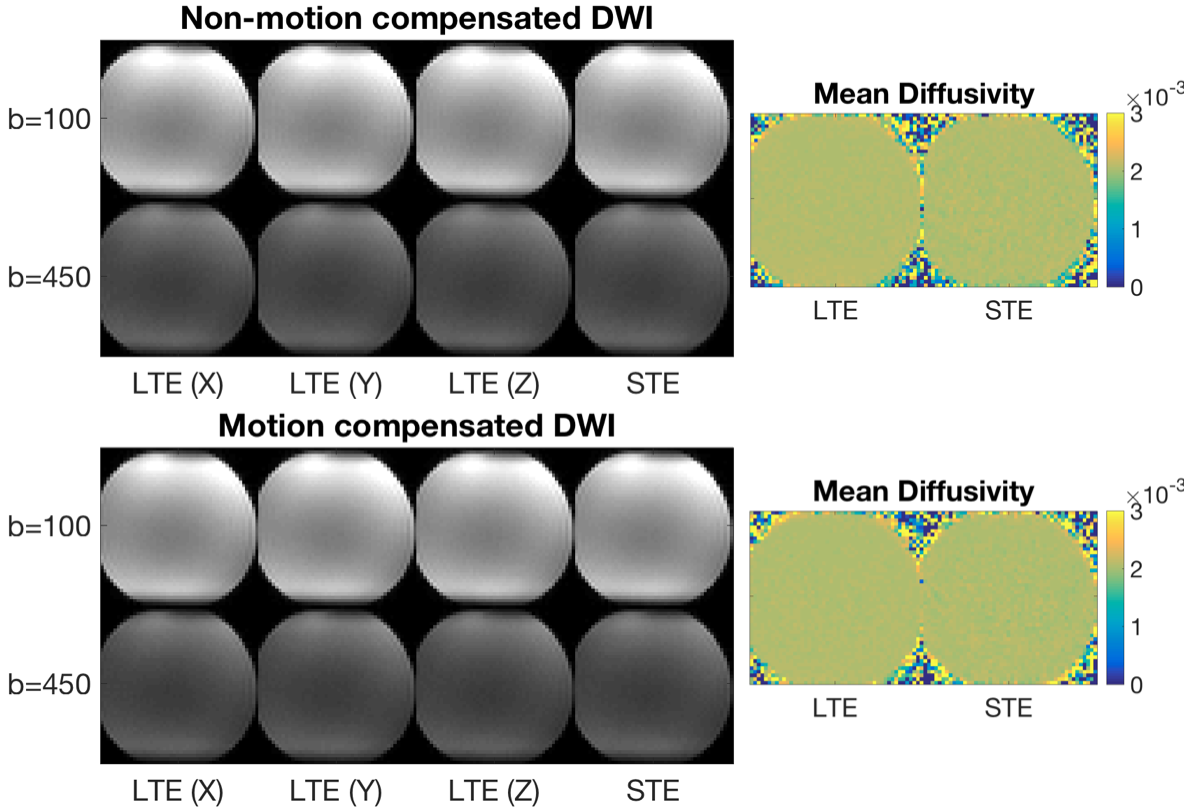
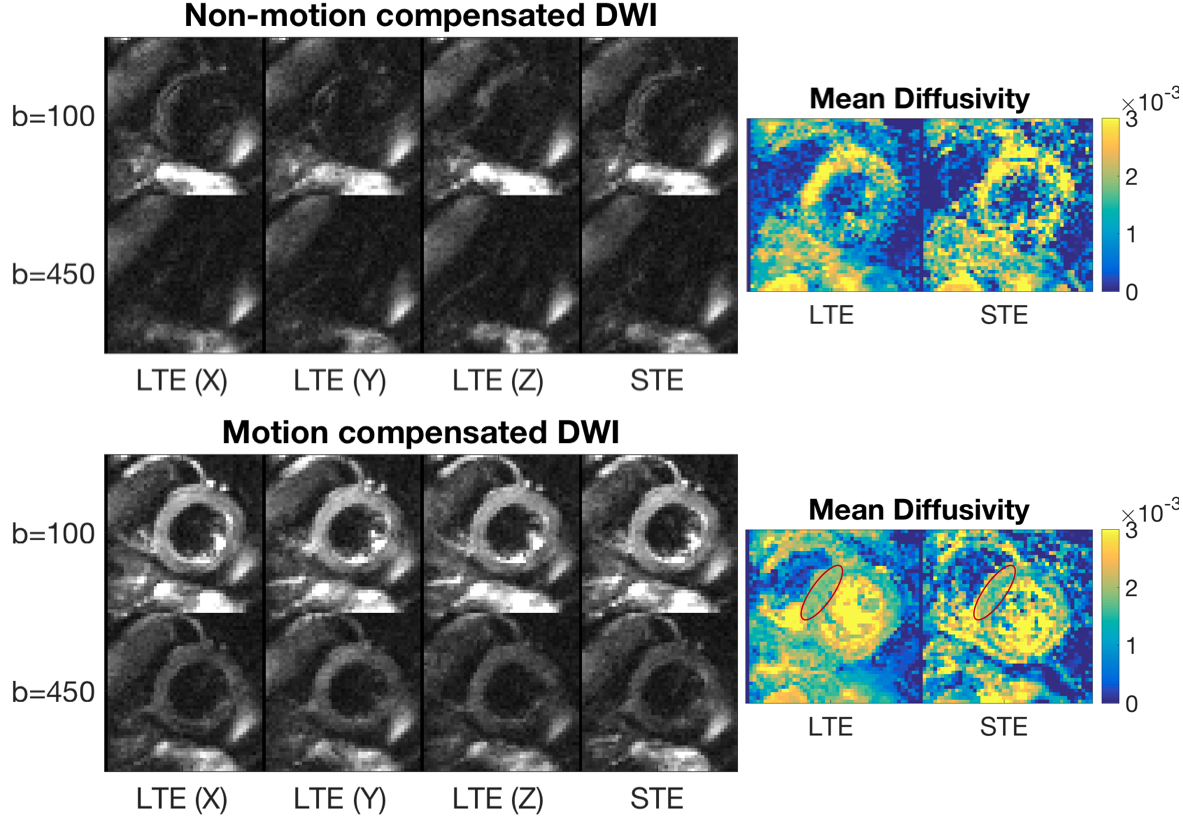
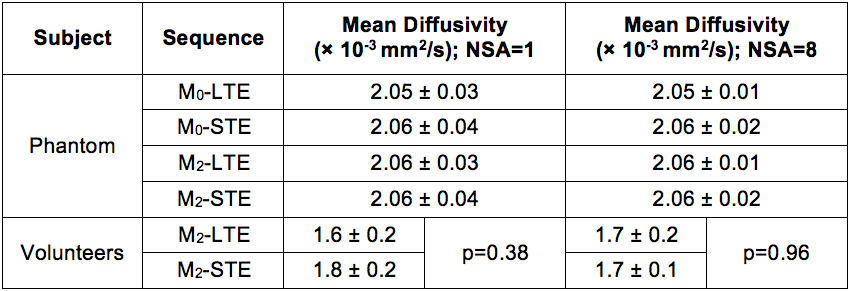
Analysis of Maxwell terms shows that the M2-LTE and M2-STE sequences are fully compensated with respect to concomitant gradients. This is corroborated by the phantom DW images and MD maps across different phantom positions and slice orientations, with representative phantom data shown (Figure 1). Without motion compensation, DW images and MD maps from a healthy volunteer exhibit complete signal dropout due to motion (Figure 2). In the phantom, all waveforms yielded an MD of approximately 2.06×10-3mm2/s (Table 1). The MD in the left ventricular septal wall in healthy volunteers was (mean±SD across subjects) 1.7×10-3± 0.2×10-3mm2/s (M2-LTE) and 1.7×10-3± 0.1×10-3mm2/s (M2-STE) for NSA=8, and the differences were not significant (p=0.96; two-tailed t-test). Similar results were observed for NSA=1 (Table 1).Discussion
We have demonstrated a method that yields isotropic diffusion encoding but no velocity or acceleration encoding. In addition, it suffers no effects due to concomitant gradients. This facilitates robust and efficient CDWI with the prospect of reducing acquisition times by a factor of 3, thereby improving the feasibility of fast sub-minute MD mapping in patient cohorts. We show that an acquisition time of 6 s (NSA=1; STE) is possible. However, the use of NSA > 1, as adopted in CDWI studies in general, improves robustness to cardiac motion. Efficient isotropic encoding was enabled by the use of asymmetric diffusion waveforms, but these may give rise to non-zero net concomitant fields and consequent spatially varying gross signal loss. Such effects can be cancelled by correction gradients if the slice orientation is known a priori, but this is not the case in CDWI. Inherent immunity to concomitant fields is therefore valuable, and precludes the need for separate and potentially incomplete correction. The method would apply as well in other body imaging (eg. liver or kidney) where bulk motion can be problematic.Acknowledgements
This work was supported by the British Heart Foundation, UK (SI/14/1/30718). The authors thank David Shelley for performing the MRI scans and Petra Bijsterveld for organising the ethics application.References
1. Wu MT, Tseng WYI, Su MYM, Liu CP, Chiou KR, Wedeen VJ, Reese TG and Yang CF. Diffusion tensor magnetic resonance imaging mapping the fiber architecture remodeling in human myocardium after infarction - Correlation with viability and wall motion. Circulation. 2006;114:1036-45.
2. Nguyen C, Lu MJ, Fan ZY, Bi XM, Kellman P, Zhao SH and Li DB. Contrast-free detection of myocardial fibrosis in hypertrophic cardiomyopathy patients with diffusion weighted cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2015;17:107.
3. Abdullah OM, Drakos SG, Diakos NA, Wever-Pinzon O, Kfoury AG, Stehlik J, Selzman CH, Reid BB, Brunisholz K, Verma DR, Myrick C, Sachse FB, Li DY and Hsu EW. Characterization of diffuse fibrosis in the failing human heart via diffusion tensor imaging and quantitative histological validation. NMR Biomed. 2014;27:1378-86.
4. Mori S, van Zijl PC. Diffusion weighting by the trace of the diffusion tensor within a single scan. Magn Reson Med. 1995;33(1):41-52
5. Wong EC, Cox RW, Song AW. Optimised isotropic diffusion weighting. Magn Reson Med. 1995;34:139-43.
6. Sjolund J, Szczepankiewicz F, Nilsson M, Topgaard D, Westin CF and Knutsson H. Constrained optimization of gradient waveforms for generalized diffusion encoding. J Magn Reson. 2015;261:157-68.
7. Baron CA, Lebel RM, Wilman AH, Beaulieu C. The effect of concomitant gradient fields on diffusion tensor imaging. Magn Reson Med. 2012;68(4):1190-201.
8. Szczepankiewicz F and Nilsson M. Maxwell-compensated waveform design for asymmetric diffusion encoding, In: Proceedings of the 26th Annual Meeting of the International Society for Magnetic Resonance in Medicine, Paris, France, 2018.
9. von Deuster C, Stoeck CT, Genet M, Atkinson D, Kozerke S. Spin Echo Versus Stimulated Echo Diffusion Tensor Imaging of the In Vivo Human Heart, Magn Reson Med. 2016;76(3):862-72.
10. Klein S, Staring M, Murphy K, Viergever MA and Pluim JPW. elastix: a toolbox for intensity based medical image registration. IEEE Trans on Med Imag. 2010;29(1):196-205.
Figures