2034
Optimisation of diffusion encoding schemes for in vivo cardiac DTI1University of Leeds, Leeds, United Kingdom, 2Massachusetts General Hospital, Harvard Medical School, Cardiovascular Research Center, Martinos Center for Biomedical Imaging, Charlestown, MA, United States, 3Cedars-Sinai Medical Center, Biomedical Imaging Research Institute, Los Angeles, CA, United States, 4Division of Cardiovascular Medicine, Radcliffe Department of Medicine, University of Oxford, Oxford, United Kingdom
Synopsis
Cardiac diffusion tensor imaging (CDTI) measurements are sensitive to a range of imaging parameters including the number of signal averages (NSA) and the number of unique diffusion-weighting directions (ND). However, there is no clear guidance on their specifications for clinical imaging. We evaluated the impact of ND and NSA on the accuracy and precision of the mean diffusivity, fractional anisotropy and helix angle in 10 healthy volunteers. Our findings support the need for standardisation of CDTI protocols to facilitate inter-study and inter-site comparison of data, and definition of clinically relevant thresholds for catalysing the clinical adoption of CDTI.
Purpose
In vivo cardiac diffusion tensor imaging (CDTI) is a rapidly emerging technique for contrast-free myocardial tissue characterisation. It is challenging for several reasons including cardiac motion. In order to obtain adequate signal-to-noise ratio (SNR) and minimise artefacts, imaging protocols typically employ high numbers of signal averages (8 ≤ NSA ≤ 16).1,2,3 However, the number of unique directions of diffusion-weighting (6 ≤ ND ≤ 12)1,2,3,4,5 remains small relative to DTI protocols used in other anatomy e.g. brain. Previous work ex vivo quantified the effects of SNR, ND and spatial resolution on CDTI parameters such as mean diffusivity (MD), fractional anisotropy (FA) and helix angle (HA).6 However, there is currently no clear guidance or standardisation in terms of NSA or ND for clinical imaging. We present a systematic evaluation of the accuracy and precision of CDTI parameters as a function of NSA and ND.Methods
In vivo CDTI data were acquired in healthy volunteers (N=10) on a Prisma 3T MRI scanner (Siemens Healthineers, Erlangen, Germany). All volunteers provided written consent under approved ethics. A single-shot spin echo EPI sequence with 2DRF inner volume excitation and cardiac triggering was used: TR = 3 RR-intervals, TE = 82 ms, field-of-view = 320 x 111 mm2, in-plane resolution = 2.3 x 2.3 mm2, slice thickness = 8 mm, number of slices = 3, bandwidth = 2012 Hz/px, blow = 100 s/mm2 and bhigh = 450 s/mm2.7 The blow data were acquired in 3 orthogonal directions (O3) with NSA = 8 (i.e. O3B100NSA8), whereas the reference dataset used O3B100NSA24. Three diffusion schemes were employed for bhigh: Jones6 (J6)8 and Dual6 (D6)9 representing common diffusion schemes, and Caruyer144 (C144)10 with the numbering representing ND. The Caruyer scheme was designed to provide incremental angular distribution. We could therefore downsample C144 in post-processing to C24, C32, C48 and C96 by considering only the first ND directions, whilst maintaining a relatively even distribution of diffusion-weighting (DW) directions. Multiple repetitions were acquired and averaged in post-processing to yield 1 ≤ NSA ≤ 16 (J6 and D6) and 1 ≤ NSA ≤ 4 (C12 to C144). All magnitude image data were affinely registered in 2D using Elastix.11 The LV myocardium was manually segmented, and tensors were fitted to the DTI data without prior averaging, using non-linear least squares. Maps of MD, FA, and HA were calculated in Matlab (Mathworks, Natick, USA). Accuracy was reported as the root mean squared error (RMSE) with respect to the reference O3B100NSA24 + C144B450NSA4 dataset, averaged across the LV myocardium. Uncertainty was evaluated by bootstrapping to generate 1000 DTI datasets, and 95% confidence intervals were reported.Results
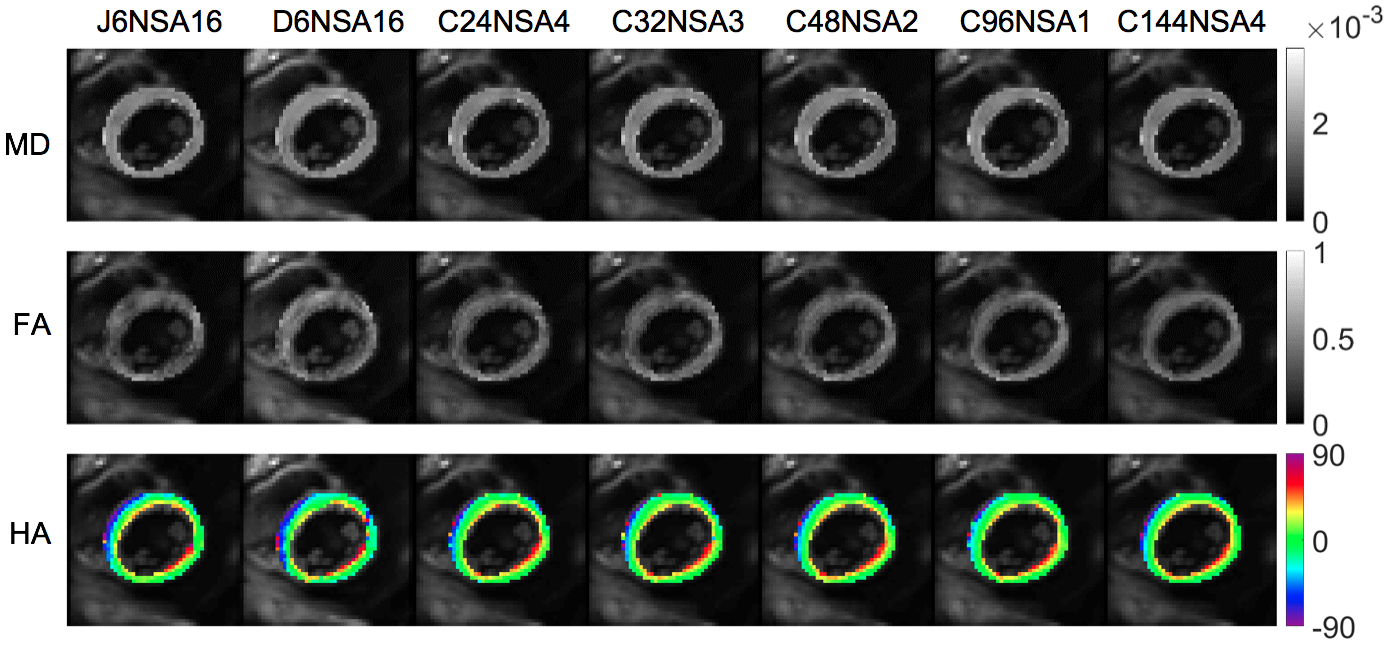
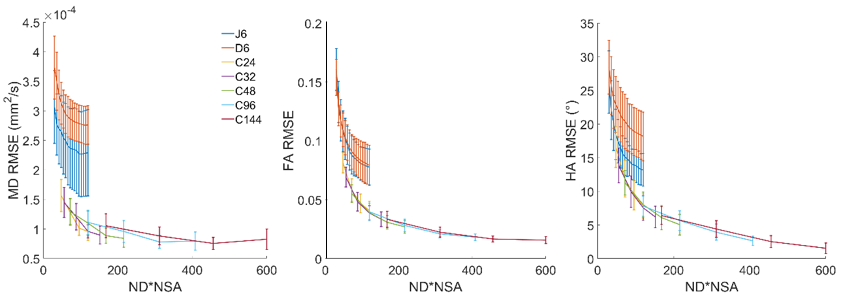
Representative CDTI parameter maps using various configurations of ND and NSA are given in Figure 1. Plots of accuracy vs ND*NSA show that there are considerable differences in results depending on the diffusion scheme used (Figure 2). In J6NSA16 for example, the mean RMSE of MD, FA and HA was 2.29 × 10-4mm2/s, 0.08 and 13.2°, whereas the C96NSA1 dataset yielded values of 1.11 × 10-4mm2/s, 0.04 and 7.8° respectively. Uncertainty in all parameters was clearly reduced as ND increased from 6 to 144 when considering only NSA = 1 (Figure 3). In the time-normalised experiments where ND*NSA were equal, we found that the uncertainty of MD, FA and HA are modestly reduced with higher ND (Figure 4).Discussion
We observed that the accuracy and precision of the CDTI parameter estimation improves with increasing ND and NSA. However, the markedly poorer accuracy of the J6 and D6 schemes despite averaging up to NSA = 16 suggests potential fundamental issues such as (i) inadequate angular resolution in DW causing systematic bias, and (ii) different eddy current behaviour that cannot be recovered by averaging. This complicates quantitative comparison between datasets acquired with different ND and NSA. Precision in CDTI parameters is improved by prioritising ND over NSA for a given acquisition time. Our findings motivate the standardisation of ND and NSA, among other imaging parameters, to define clinically relevant thresholds in measured parameters and catalyse clinical uptake of CDTI.Acknowledgements
This work was supported by the British Heart Foundation, UK (FS/11/50/29038). The authors thank David Shelley for performing the MRI scans, and Petra Bijsterveld for arranging the ethics approvals.References
1. von Deuster C, Stoeck CT, Genet M, Atkinson D, Kozerke S. Spin Echo Versus Stimulated Echo Diffusion Tensor Imaging of the In Vivo Human Heart, Magn Reson Med. 2016;76(3):862-72.
2. Stoeck CT, von Deuster C, Genet M, Atkinson D, Kozerke S. Second-Order Motion-Compensated Spin Echo Diffusion Tensor Imaging of the Human Heart, Magn Reson Med. 2016;75:1669-76.
3. Scott AD, Ferreira P, Nielles-Vallespin S, Gatehouse P, McGill LA, Kilner P, Pennell DJ, Firmin DN. Optimal Diffusion Weighting for In Vivo Cardiac Diffusion Tensor Imaging, Magn Reson Med. 2015;74:420–30
4. Moulin K, Croisille P, Feiweier T, Delattre BM, Wei H, Robert B, Beuf O, Viallon M. In vivo free-breathing DTI and IVIM of the whole human heart using a real-time slice-followed SE-EPI navigator-based sequence: a reproducibility study in healthy volunteers. Magn Reson Med. 2016;76:70–82.
5. Welsh CL, DiBella EVR, Hsu EW. Higher-Order Motion-Compensation for In Vivo Cardiac Diffusion Tensor Imaging in Rats, IEEE Trans Med Imag. 2015;34(9):1843-53.
6. McClymont D, Teh I, Schneider JE. The impact of signal-to-noise ratio, diffusion-weighted directions and image resolution in cardiac diffusion tensor imaging – insights from the ex-vivo rat heart. J Cardiovasc Magn Reson. 2017;19:90.
7. Nguyen C, Ma S, Bi X, Li D. Towards High Success Rate in vivo Cardiac DTI on a Clinical 3T Scanner: Considerations on Heart Rate, Body-to-Mass Index, and Free Breathing. In: Proceedings of the 26th Annual Meeting of ISMRM, Honolulu, USA, 2017, p2721.
8. Jones DK, Horsfield MA, Simmons A. Optimal Strategies for Measuring Diffusion in Anisotropic Systems by Magnetic Resonance Imaging, Magn Reson Med. 1999;42:515–25.
9. Davis TL, Wedeen VJ, Weisskoff, Rosen BR. White matter tract visualization by echo-planar MRI. In: Proceedings of the 12th Annual Meeting of SMRM, New York, 1993, p289.
10. Caruyer E, Lenglet C, Sapiro G, Deriche R. Design of multishell sampling schemes with uniform coverage in diffusion MRI, Magn Reson Med. 2013;69(6):1534-40.
11. Klein S, Staring M, Murphy K, Viergever MA and Pluim JPW. "elastix: a toolbox for intensity based medical image registration," IEEE Trans on Med Imag. 2010;29(1):196-205.
Figures