2029
3D whole-heart dark-blood late gadolinium enhancement without additional magnetization preparation for simultaneous detection of both atrial and ventricular fibrosis1Maastricht University Medical Centre, Maastricht, Netherlands
Synopsis
Accurately acquiring the location and extent of thin atrial fibrosis patterns demands for improved imaging techniques compared to conventional ventricular LGE. Recently, we developed a novel 2D dark-blood LGE approach that significantly increases scar-to-blood contrast without using additional magnetization preparation. In this feasibility study, we sought to translate this novel approach towards 3D fibrosis imaging for simultaneous detection of both atrial and ventricular scar. 3D dark-blood PSIR LGE proves to be a readily available approach for detection of both atrial and ventricular fibrosis, with improved robustness for arrhythmias, increased scar-to-blood contrast, improved patient comfort, and enabling a more versatile analysis.
Background
Late gadolinium enhancement (LGE) is a widely used CMR technique to non-invasively assess myocardial fibrosis. Over the years the clinical utility of LGE has widened and effort has been put into the detection of thin atrial fibrosis. Atrial fibrosis is expected to play a crucial role in the occurrence of cardiac arrhythmias.[1] Recently, more focus is placed on investigating whether the location and extent of the fibrosis patterns can predict the chance of success for subsequent atrial ablation therapy.[2] Accurately acquiring the location and extent of atrial fibrosis patterns in patients with atrial fibrillation demands for improved imaging techniques compared to conventional LGE used for ventricular fibrosis. Imaging such patients requires dedicated pulse sequences that are more robust for cardiac arrhythmias, while increased resolution and improved image contrast are required to detect the thin fibrosis patterns. Furthermore, 3D coverage is preferred over thick 2D slices to enable multiplanar reconstructions for optimal analysis and to create an anatomical map of the atria to guide subsequent ablation therapy.
Recently, we developed a novel 2D dark-blood LGE approach that significantly increases scar-to-blood contrast without using additional magnetization preparation.[3] The combination of phase-sensitive inversion-recovery (PSIR) and nulling the LV blood pool, instead of viable myocardium, provides an opportunity to suppress the blood signal whilst preserving the bright scar signal, and thereby increasing the conspicuity of thin subendocardial scar patterns. This new approach was evaluated in a large cohort of 300 patients and showed improved detection of ischaemic scar compared to conventional LGE, with increased observer confidence and improved image quality.[4]. In this feasibility study, we sought to translate this novel approach towards 3D fibrosis imaging in patients with atrial fibrillation.
Methods
15 consecutive patients referred for atrial ablation therapy were enrolled and scheduled for an additional MRI examination before therapy on a 1.5T scanner (Ingenia, Philips Healthcare, Netherlands). Functional 2-chamber, 4-chamber, and short-axis cine imaging was performed, followed by an intravenous injection of 0.2 mmol/kg gadobutrol (Gadovist, Bayer, Germany). Ten minutes after injection, dark-blood LGE imaging was performed using a 3D whole-heart phase-sensitive inversion recovery, respiration navigated, ECG-gated, turbo field echo pulse sequence. Typical acquisition parameters were: free-breathing using navigator gating, a transverse whole-heart imaging volume with voxel size = 1.25×1.25×2 mm (reconstructed to 0.65×0.65×1 mm), TR/TE=6.6/3.2 ms, flip angle=25°, SENSE factors 2.25 (in-plane) and 1.5 (out-of-plane). Data was only acquired during the diastolic phase of the cardiac cycle using ECG gating. The exact period of diastasis (130ms maximum) was determined using the earlier acquired 4-chamber cine image. A preceding Look-Locker scan (TI-scout) was used to determine the inversion time for nulling the LV blood. 30ms was added to compensate for the increase in inversion time due to contrast washout during the scan duration. Spectral suppression was used to suppress the fat signal. Typical scan time was 15–25 minutes depending on the subject's respiratory and heart rate. For all patients, the 3D dark-blood PSIR LGE scan was visually analyzed for overall image quality in terms of resolution, dark-blood contrast, and potential image artefacts. All LGE scans showing diagnostic quality were analyzed for the presence of both atrial and ventricular fibrosis.
Results
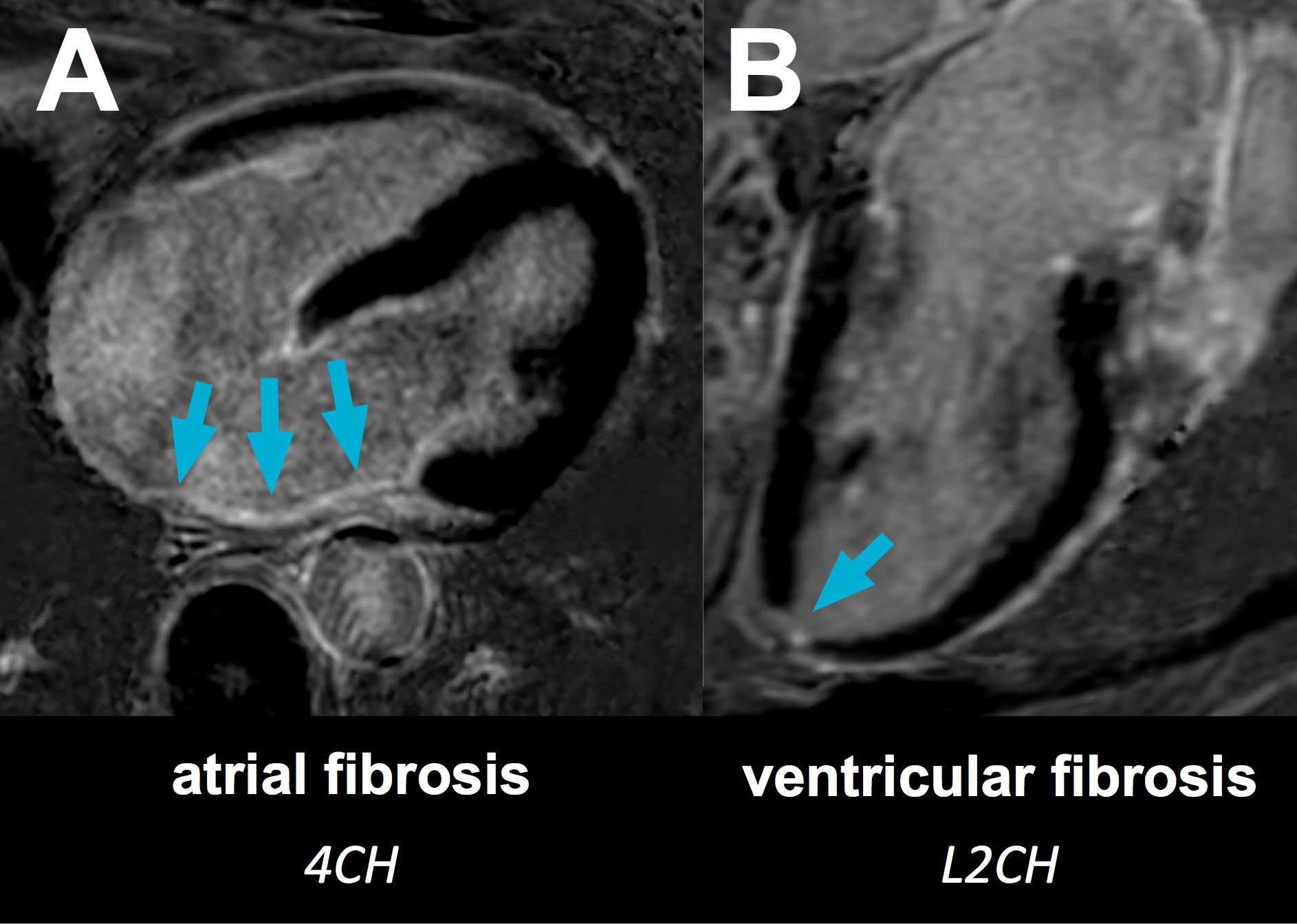
Complete 3D dark-blood PSIR LGE datasets were successfully acquired in 14 patients, while one patient left the scanner prematurely after contrast injection. One patient was excluded from further analysis due to breathing motion artefacts. All remaining datasets (n=13) showed the desired dark-blood PSIR effect and good to excellent diagnostic image quality. Atrial fibrosis and ventricular fibrosis was observed in nine (69%) and four (21%) patients, respectively (figure 1). Six patients (46%) showed atrial fibrillation during data acquisition.
Discussion
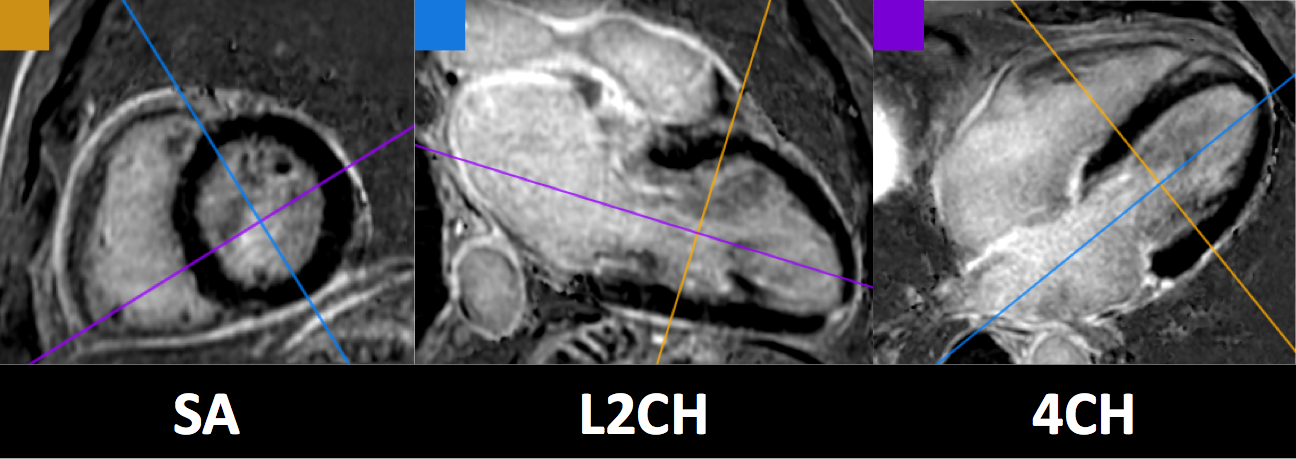
3D dark-blood PSIR LGE is a readily available approach for detection of both atrial and ventricular fibrosis. Combining the novel dark-blood effect, which significantly increases scar-to-blood contrast, with a high-resolution 3D acquisition, enables detection of thin atrial fibrosis patterns, while the two-beat PSIR acquisition scheme proves to be robust when imaging patients with ongoing arrhythmias. Whole-heart 3D coverage allows for simultaneous detection of both atrial and ventricular fibrosis in a single acquisition, enables analysis in any desired imaging plane after acquisition (figure 2), and creates an anatomical map of the atria to guide subsequent ablation therapy (no CT-scan required anymore). Furthermore, by using a respiratory navigated free-breathing acquisition, rather than multiple breath-hold acquisitions, patient comfort is increased and new opportunities arise for patients with shortness of breath. As no additional magnetization preparation is required for this novel method, clinical application on current MR systems is readily available without the need for extensive optimizations, software modifications, and/or additional training.
Acknowledgements
NoneReferences
1. Burstein B, Nattel S. Atrial Fibrosis: Mechanisms and Clinical Relevance in Atrial Fibrillation. JACC 2008
2. Akoum N, Daccarett M, McGann C, et al. Atrial Fibrosis Helps Select the Appropriate Patient and Strategy in Catheter Ablation of Atrial Fibrillation: A DE-MRI Guided Approach. J Cardiovasc Electrophysiol 2011
3. Holtackers RJ, Chiribiri A, Schneider T, et al. Dark-blood late gadolinium enhancement without additional magnetization preparation. J Cardiovasc Magn Reson 2017
4. Holtackers RJ, van de Heyning CM, Nazir MS, et al. Clinical value of dark-blood late gadolinium enhancement without additional magnetization preparation. Proc Intl Soc Mag Reson Med 2018
Figures