2026
The structural basis for haemodynamically compromising VT assessed using high-resolution late gadolinium enhanced cardiovascular magnetic resonance imaging under contrast steady state1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Abbott, Minneapolis, MN, United States, 3King's College London, London, United Kingdom, 4Siemen's healthcare, London, United Kingdom, 5Guy's and St Thomas' NHS Foundation Trust, London, United Kingdom
Synopsis
Using a translational porcine model, the structural basis for post myocardial infarction ventricular tachycardia was assessed using in-vivo cardiac magnetic resonance imaging. High-resolution LGE imaging was acquired under contrast steady state in order to allow detailed tissue characterisation. Arrhythmia was induced and assessed under haemodynamic support to allow the unambiguous identification of arrhythmogenic tissue involved in these scar mediated VT circuits. The electrophysiological and imaging data was then registered to establish the structural features of tissue involved in these rhythms. It was identified that tissue participating in the diastolic phase of post-MI VT was thinner, had non-transmual scar or intermediate signal intensity and had higher gradients in tissue thickness.
Introduction
The majority of post myocardial infarction (MI) ventricular tachycardia’s (VT) are reentrant in nature with circuits are localised within viable tissue existing in close proximity to dense scar(1). Identifying arrhythmogenic tissue responsible for post myocardial infarction (MI) ventricular tachycardia (VT) is a prerequisite for the delivery of ablative therapy to destroy this tissue. Classical descriptions of VT were based on observations of haemodynamically tolerated VT often made in the context of LV aneurysm(2). Emergency and secondary prevention therapy for MI has increased the incidence of haemodynamically compromising VT and reduced the incidence of LV aneurysm, emphasising the need to identify the structural basis of haemodynamically compromising VTs. This experiment aimed to establish the structural basis for haemodynamically compromising post-MI VT.Methods
7 pigs with healed antero-septal MI were studied. Fifteen minutes after 0.1mmol/kg gadobutrol (Gd), 0.0011mmol/kg/min Gd infusion was commenced. After a further 15 minutes 1.2 x 1.2 x 1.2mm3 LGE CMR scans (SSFP; coronal orientation; linear k-space reordering; TE/TR/α: 1.58ms/3.6ms/90°; gating window = 7mm; parallel imaging using GRAPPA with an acceleration factor of 2; resolution 1.2x1.2x1.2mm3; FOV: 400 x 257 mm2) were acquired under gadolinium infusion during contrast steady state(3). Each pig underwent electrophysiology study with prophylactic VA-ECMO support. An anatomic mesh generated from the in-vivo imaging was imported and registered to the endocardial shell within the electro-anatomic mapping system (EAMS). Activation maps during sustained VT were acquired and the location of diastolic electrograms (EGMs) recorded. Tissue thickness, scar transmurality and heterogeneous tissue (HT) transmurality were calculated from the in-vivo imaging and mapped VT isthmuses were registered to LGE-CMR to allow an assessment of the structural characteristics of the tissue at these locations.Results
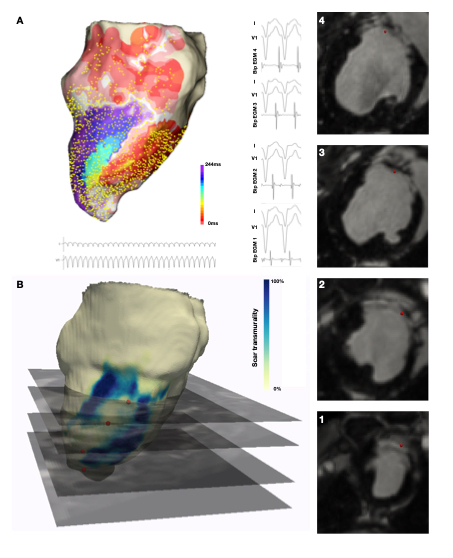
Diastolic isthmus locations (example in figure, panel A) had a mean scar transmurality of 37.4 (±36.3)% (median 29.3%, IQR 0 – 77.3%) and a mean HT transmurality of 18.3 (±22.9)% (median 7.4%, IQR 0 – 30.3%). 80.1% of diastolic isthmus locations were found within areas of non-transmural scar or HT SI. Of those diastolic isthmus locations that were in regions without scar or HT, all were within 15mm of a region of HT and 89% lay within 10mm of a region of HT. The imaging characteristics of the locations at which the diastolic isthmus occurred during the observed VTs were compared with locations at which normal EGMs were recorded. Tissue participating in the diastolic component of VT circuits was thinner than healthy tissue (median thickness isthmus = 5.5mm vs 8.2mm healthy tissue, p < 0.0001) and was closer to HT (median distance from HT isthmus tissue 2.8mm v 11.4mm healthy tissue, p < 0.0001). Non-scarred regions with diastolic activation during VT were closer to steep gradients in tissue thickness than non-scarred locations with normal EGMs (isthmus locations distance = 6.26mm (IQR 0 – 11.63mm) vs 9.67mm (IQR 2.87 – 18.56mm) for non-isthmus locations, p<0.0001).Conclusion
The diastolic component of the reentrant circuit is principally located in regions of non-transmural scar/HT. In comparison with tissue demonstrating normal EGMs, tissue harbouring the diastolic isthmus is thinner and exclusively located within 15mm of HT. A significant minority of regions with diastolic activation during VT are in locations with no scar/HT, but as well as existing in close proximity to HT these regions were frequently adjacent to steep gradients in tissue thickness.Acknowledgements
No acknowledgement found.References
1. Stevenson WG, Khan H, Sager P, Saxon LA. Identification of Reentry Circuit Sites During Catheter Mapping and Radiofrequency Ablation of Ventricular Tachycardia Late After Myocardial Infarction. Circulation. 1993;88:1647–70.
2. Josephson ME, Horowitz LN, Farshidi a, Kastor J a. Recurrent sustained ventricular tachycardia. 1. Mechanisms. Circulation. 1978;57(3):431–40.
3. Flett AS, Hayward MP, Ashworth MT, Hansen MS, Taylor AM, Elliott PM, et al. Equilibrium contrast cardiovascular magnetic resonance for the measurement of diffuse myocardial fibrosis: Preliminary validation in humans. Circulation. 2010;122(2):138–44.
Figures