2021
Optimizing native T1-based detection of chronic myocardial infarctions at 3T: Influence of MOLLI flip angle on the relative myocardium-to-blood T1 contrast1Biomedical Imaging Research Institute, Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2UCLA David Geffen School of Medicine, Los Angeles, CA, United States
Synopsis
Prior studies have shown that native T1 mapping at 3T provides an effective non-contrast approach for characterizing the presence and transmurality of chronic myocardial infarctions. The underlying mechanism is likely a combination of T1/T2 and magnetization transfer (MT) effects. The choice of flip angle is known to significantly affect the degree to which MOLLI-based T1 maps are confounded by MT and T2 effects. With the motivation to optimize the performance of MOLLI T1 mapping for detection of subendocardial infarcts, we hypothesized that increasing the flip angle beyond the conventionally-used 35° will provide a higher relative contrast and contrast-to-noise ratio between the infarcted myocardium and adjacent bloodpool.
Background
Prior studies have shown that native T1 mapping at 3T provides an effective non-contrast approach for characterizing the presence and transmurality of chronic myocardial infarctions.1,2 The underlying mechanism is likely a combination of T1/T2 and magnetization transfer (MT) effects.3 The choice of flip angle (FA) is known to significantly affect the degree to which T1 maps acquired using the clinically-used modified Look-Locker inversion recovery (MOLLI) acquisition are confounded by MT and T2 effects.3,4 However, the native T1 in the left ventricular bloodpool is not affected nearly as much as the myocardial native T1 by MT effects given the significantly lower MT ratio for blood compared to tissue at 3T. Therefore, by modulating the MT effects (increasing the FA) one can potentially increase the relative myocardium-to-bloodpool native T1 contrast, thereby improving the ability to detect small subendocardial infarctions on the basis of MOLLI native T1 maps.Purpose
With the motivation to optimize the performance of MOLLI T1 mapping for detection of subendocardial infarcts, we hypothesized that increasing the FA beyond the conventionally-used 35° will provide a higher relative contrast and contrast-to-noise ratio (CNR) between the infarcted myocardium and adjacent bloodpool.Methods
A phantom study was performed using a freshly-excised pig heart to verify the significant difference between the MT-induced MOLLI T1 change as a function of the FA in the myocardium vs. saline. Next, 10 farm pigs underwent occlusion of the left anterior descending artery and were reperfused after 90 minutes. Follow-up imaging studies were performed 8 weeks later on a clinical 3T scanner. Presence and extent of infarction were identified on the basis of late gadolinium enhancement (LGE) images. In each pig, one short-axis slice was selected (mid-basal) and MOLLI native T1 maps with 3 different FAs were acquired (FA = 22°, 35°, 48°). The MOLLI sequence used 6 recovery heartbeats to ensure heart-rate independence (in-plane resolution: 1.6x1.6 mm2). For the acquired short-axis slice, 3 regions-of-interest were identified based on the LGE signal intensity: (i) infarcted myocardium, using the “mean + 5 standard-deviation (SD)” criterion; (ii) adjacent bloodpool, by selecting LV cavity pixels bordering the infarct; (iii) remote myocardium, from a region showing no hyperintensity. The three identified regions were then applied to each of the three native T1 maps to calculate the infarct-versus-blood "relative T1 contrast” and the infarct-versus-blood T1-CNR defined as (T1infarct – T1blood) ÷ T1blood and (T1infarct – T1blood) ÷ SD(T1blood), respectively, where T1 refers to the MOLLI native T1 values.
Results
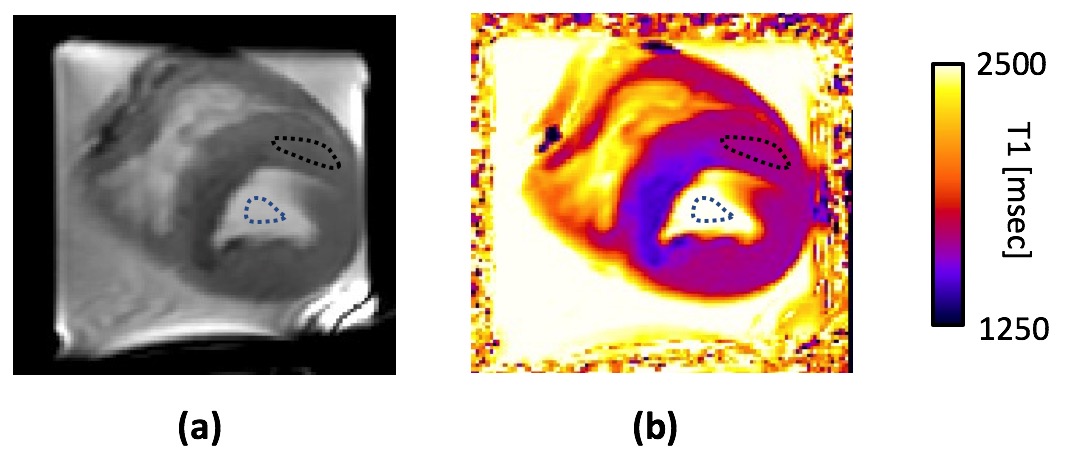
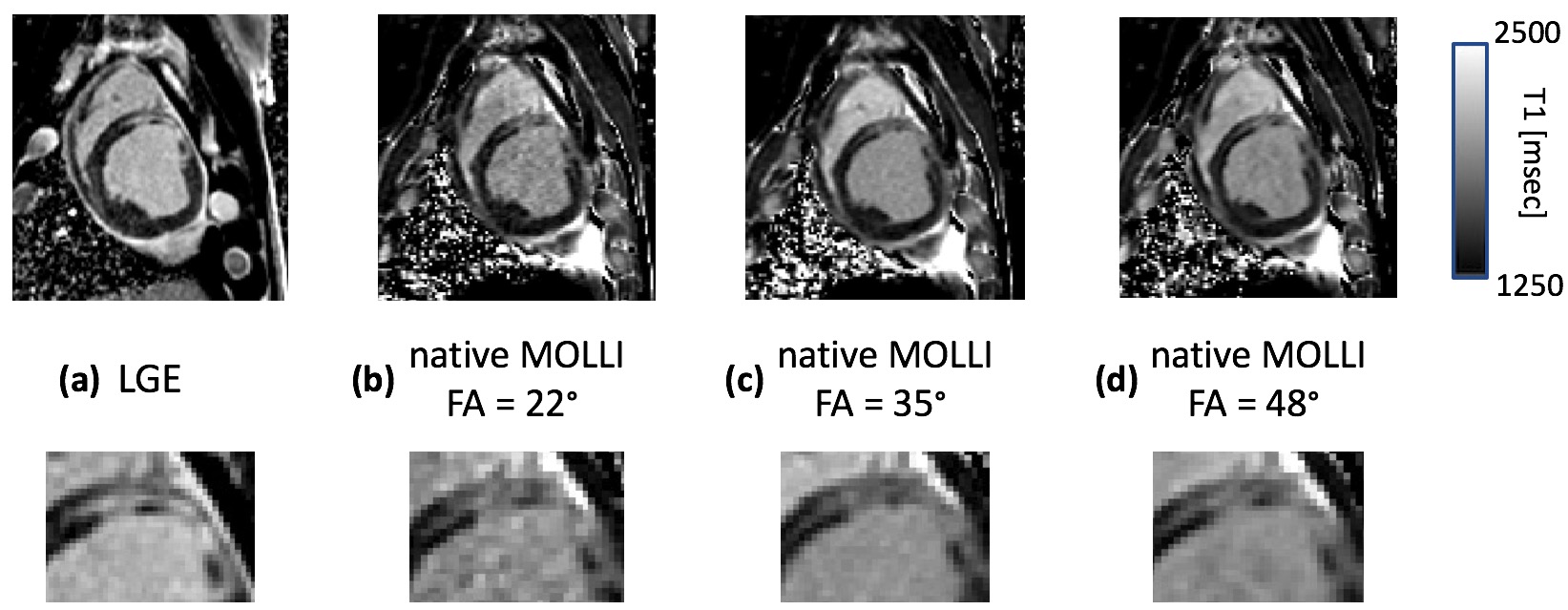
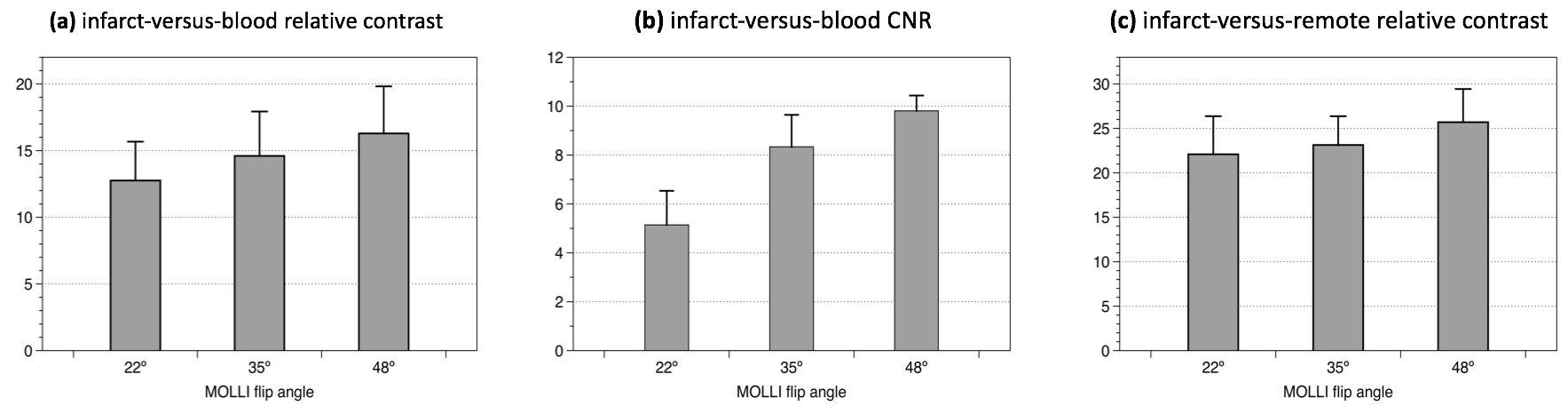
The phantom study (Fig. 1) verified that the myocardial native T1 changes significantly when FA is increased (5.5% decrease when FA is increased from 35° to 70°) whereas the bloodpool T1 remained nearly unchanged (0.2% increase). Figure 2 shows native T1 maps for the 3 FAs and the corresponding LGE image in a representative study. As can be seen in Fig. 2, the native T1 map corresponding to the MOLLI acquisition with a 22° FA shows a lower relative-contrast and CNR between the infarcted myocardium and adjacent left ventricular bloodpool in comparison to 35° and 48°. Furthermore, the detailed transmural pattern of the septal infarct for the image with FA of 22° is somewhat obscured due to noise and poor relative contrast. Overall, the high FA acquisition (48°) provides the best quality in comparison to the LGE image. Figures 3(a) and 3(b) summarize the comparison of T1-contrast, showing a significant gain in the infarct-versus-blood relative T1 contrast and T1-CNR using a higher FA of 48° (p < 0.01 for all plots in both panels). Figure 3(c) shows that the relative contrast between infarct versus remote myocardium was higher for the 48° map (p < 0.01).Conclusion
The presented results indicate that relative T1-contrast and T1-CNR between infarcted tissue and adjacent bloodpool increases with a higher FA. Although the studied animals had transmural infarcts, our results suggest that in clinical studies aimed at non-contrast detection of chronic myocardial infarction, a MOLLI sequence with high FA (within the feasible SAR limits, e.g., FA of 48° used in this study) may have a better sensitivity for detection of small subendocardial infarcts compared to the standard FA of 35°. Future work is needed to evaluate whether this qualitative improvement will result in improved diagnostic performance.Acknowledgements
No acknowledgement found.References
1. Kali A et al. Circulation Cardiovasc Imaging 2014;7:471-481. doi: 10.1161/CIRCIMAGING.113.001541
2. Kali A et al. JACC Cardiovasc Imaging 2015;8:1019-30. doi: 10.1016/j.jcmg.2015.04.018
3. Robson MD et al., Magn Reson Med. 2013 Sep;70(3):664-70. doi: 10.1002/mrm.24867
4. Kellman P et al. J Cardiovasc Magn Reson 2014;16:2. doi: 10.1186/1532-429X-16-2
Figures