2016
Tuning Blipped CAIPIRINHA for simultaneous multi-slice (SMS) balanced SSFP cardiac imaging1Aix-Marseille Univ, CNRS, CRMBM, Marseille, France, 2APHM, Hôpital Universitaire Timone, CEMEREM, Marseille, France, 3Siemens Healthcare SAS, Saint-Denis, France, 4APHM, Hôpital Universitaire Timone, Radiology Dept, Marseille, France
Synopsis
In this study, we used blipped-CAIPIRINHA simultaneous multi-slice (SMS) technique to 1) extend bSSFP coverage to 3 simultaneous slices and 2) apply it to cardiac T1 mapping. Tests were conducted on phantom and in six healthy volunteers. SMS blipped-CAIPIRINHA-bSSFP sensitivity to slice gap, slice thickness and pixel bandwidth was successfully established in terms of SNR. Native T1 quantification values over three levels of the heart (base, mid and apex) were reliable, accurate, and in line with the ones obtained with a regular single slice acquisition.
Introduction
Single-shot balanced steady-state free precession (SS-bSSFP) imaging is the preferred readout in cardiac MRI, notably for T1, T2 mapping and arterial spin-labelling (ASL), due to its reduced acquisition time and high SNR efficiency1. Our purpose is to use a blipped-CAIPIRINHA2,3 simultaneous multi-slice (SMS) technique to extend bSSFP coverage to 3 simultaneous slices4 (SMS3) for eventual application to T1 mapping. Blipped-CAIPIRINHA gradient-modulation is by design strongly affected by the slice thickness and distance, because the blip amplitude is inversely proportional to thickness and distance. Thus, the influence of these parameters was investigated in combination with pixel bandwidth (BW) to establish SNR sensitivity and define a combination of values that optimizes SNR and T1 quantification robustness.Methods
All experiments were performed on a 1.5T scanner (Avanto Siemens) using a 32-channel cardiac coil (InVivo). SMS and image reconstruction5 was performed using Gadgetron6.
This study was conducted in two stages:
I. Evaluate the impact of the slice thickness (ST), the slice gap (SG) and the BW variation on SMS3-bSSFP imaging.
II. Use the optimized parameters from the first stage to evaluate the accuracy of SMS3-T1 quantification. For both stages, the evaluations were performed on phantoms (A) and healthy volunteers (B).
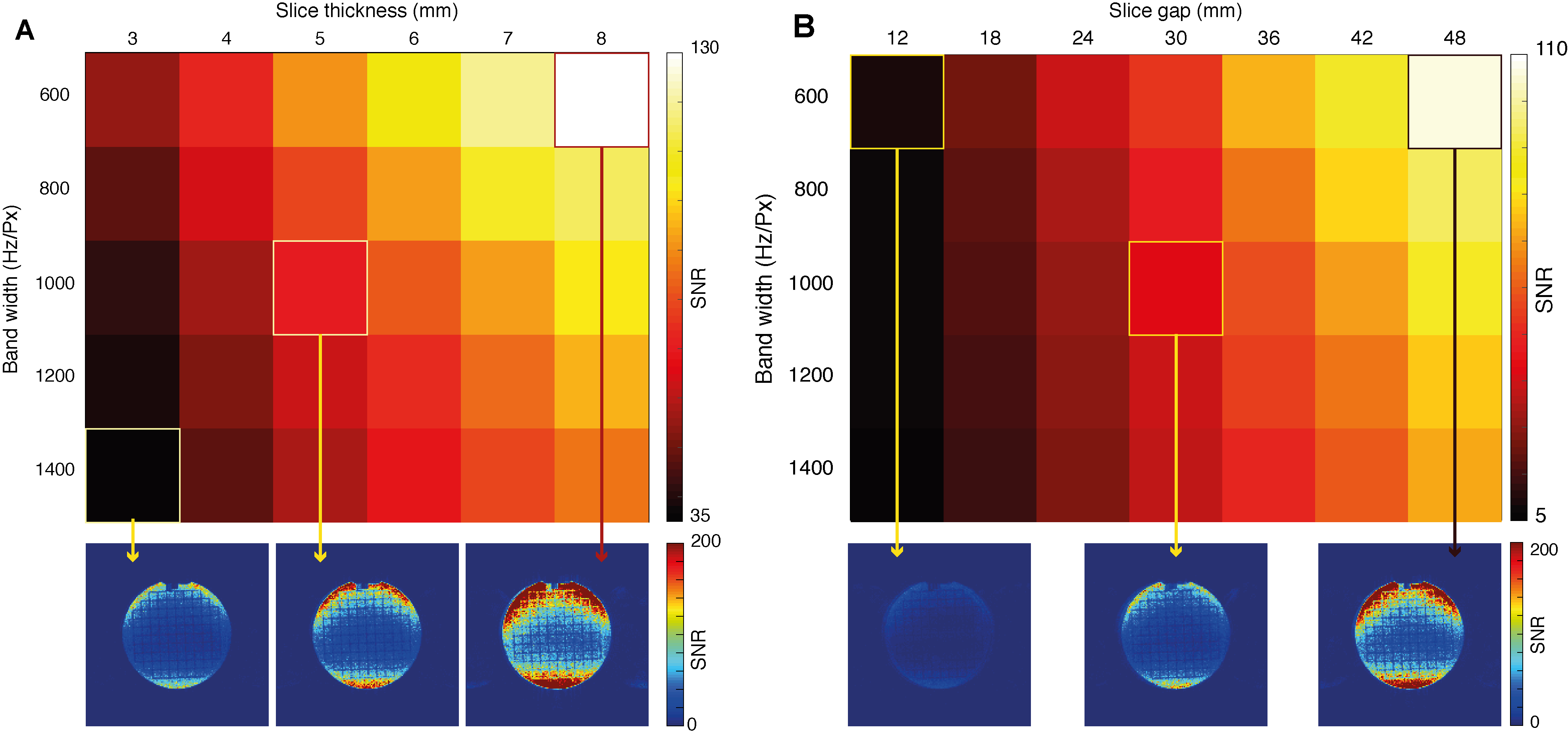
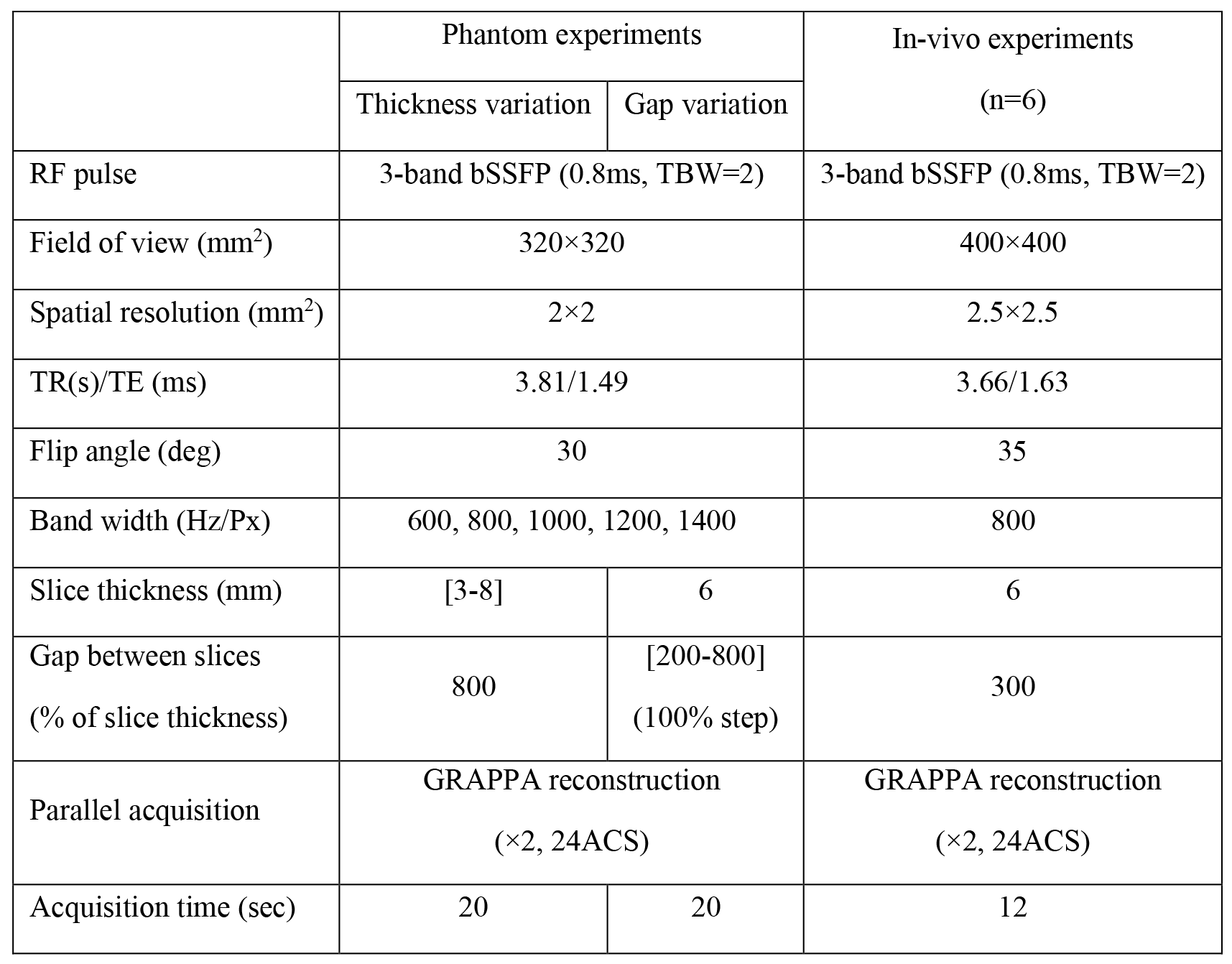
I.A.: a standardized phantom was imaged using the parameters listed in Table 1. 20 single-shot images were acquired at 1s intervals, with the transient-state (first 5) images discarded. SNR was defined as the series’ mean intensity over intensity standard deviation.
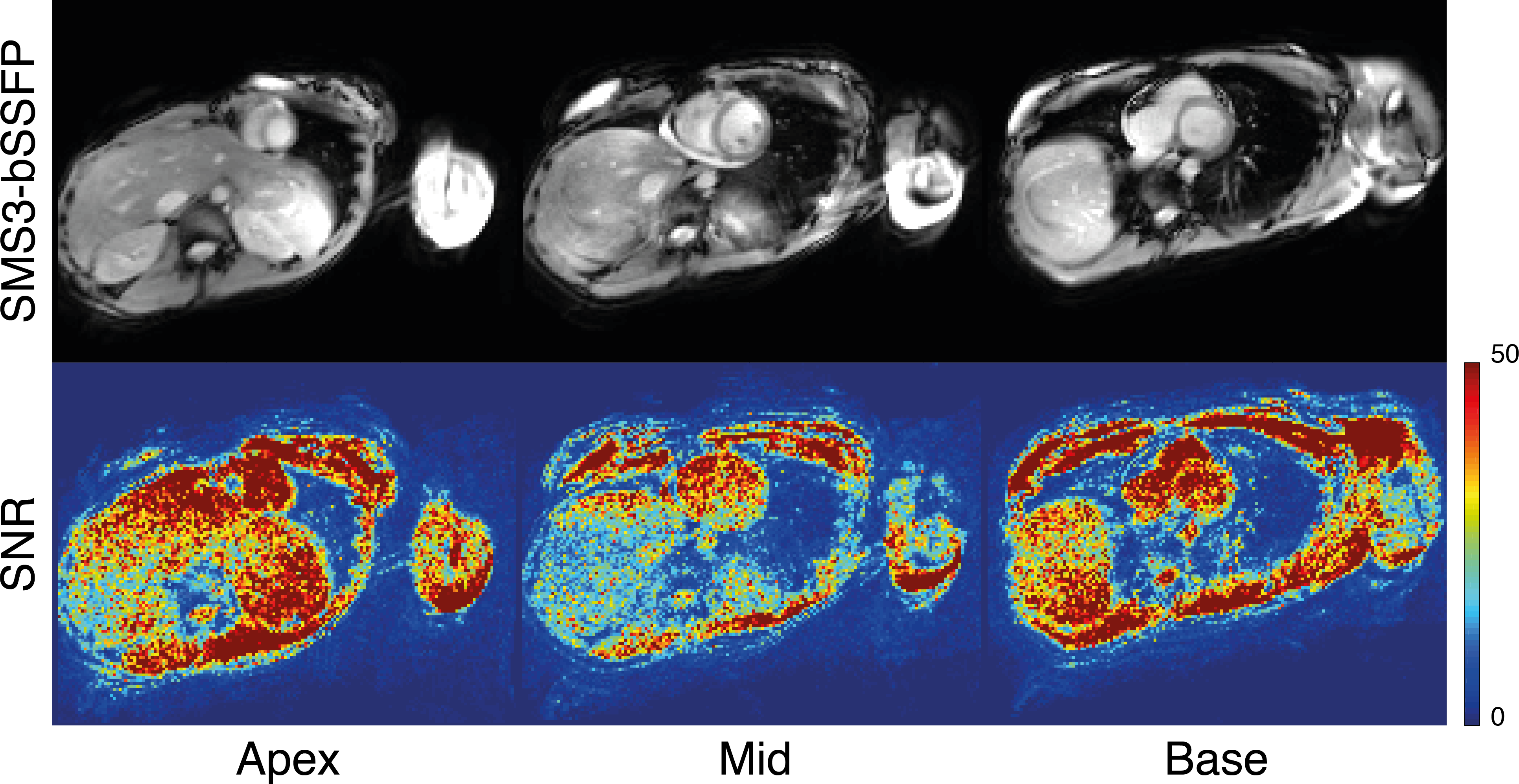
I.B.: six healthy volunteers underwent a cardiac MRI examination after providing informed consent. SMS3 single-shot bSSFP slices (basal, median and apical) were acquired with the parameters listed in Table 1.
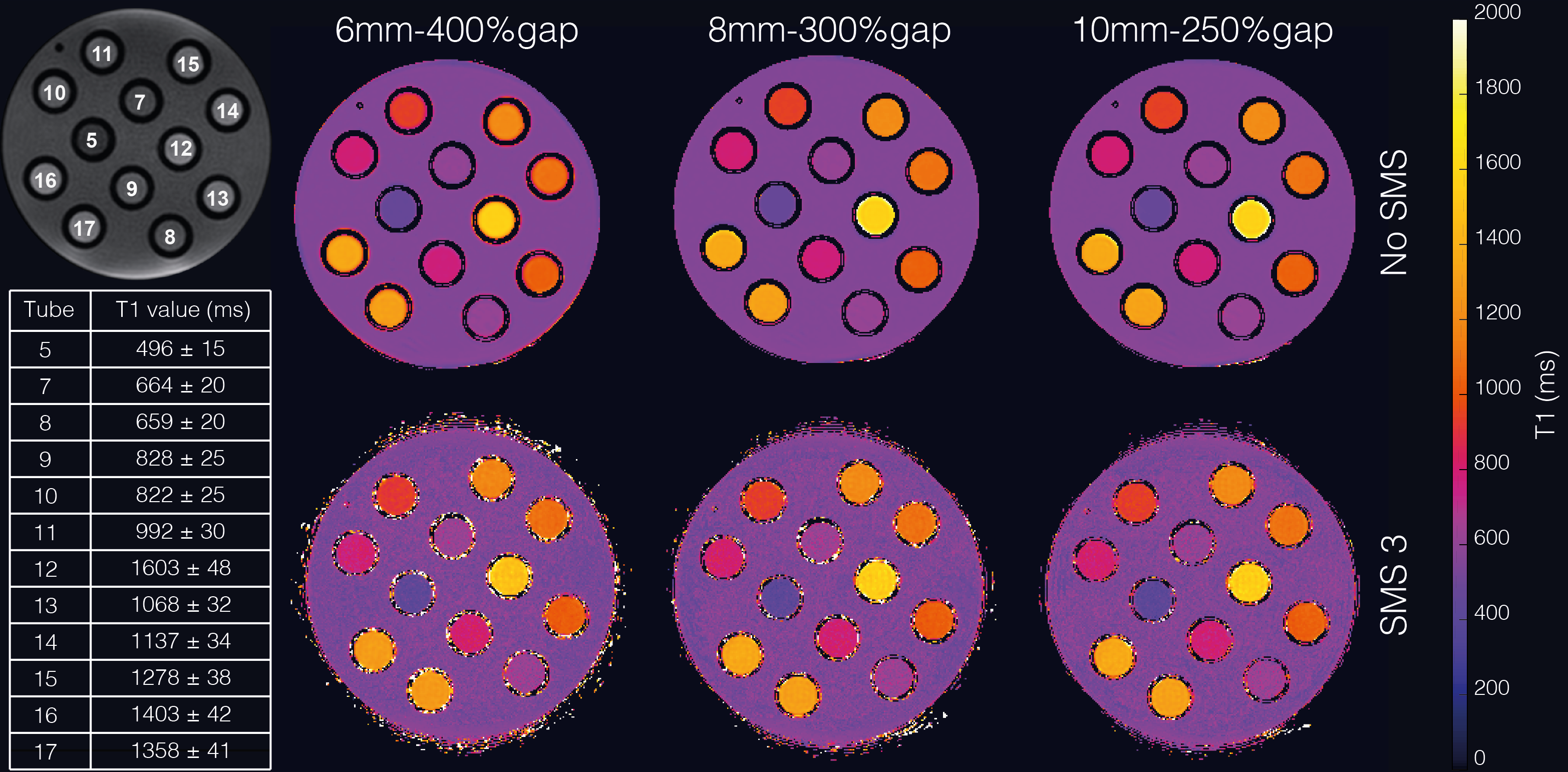
II.A.: 12 T1-calibrated Agarose gel tubes were imaged using a MOLLI 5(3)3 scheme (Fig.2). Three acquisitions with different ST and SG were performed to evaluate T1 estimation reliability. The 3 acquisitions had ST/SG of: 6/30mm, 8/21mm and 10/35mm, respectively. For all acquisitions, FOV was 300×300mm2, TE/TR/FA were 1.61ms/4.84ms/35°, pixel size was 0.94×0.94mm2 and simulated HR was 60 bpm.
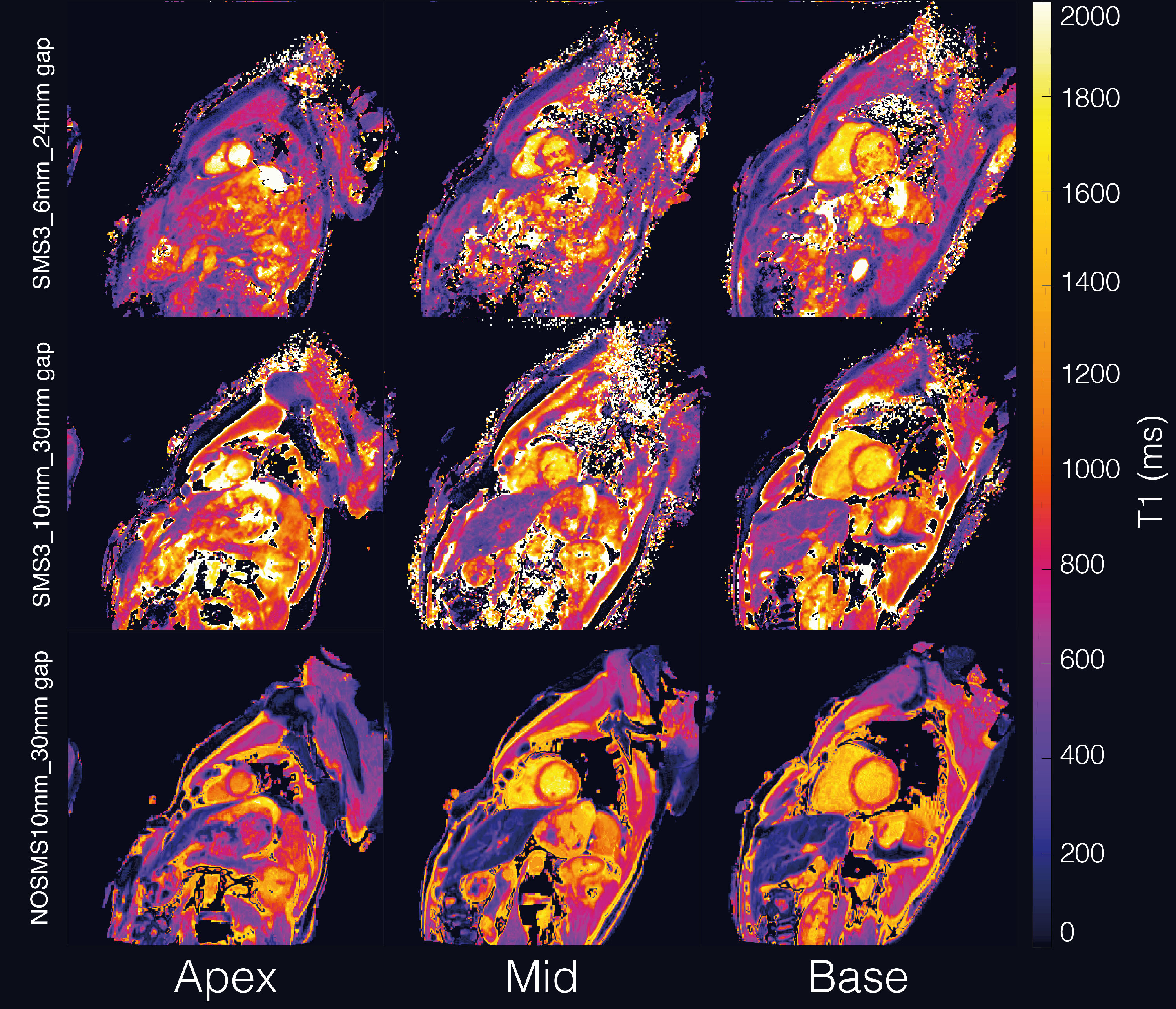
II.B.: In vivo native T1 maps were acquired using the 5(3)3 MOLLI scheme with the following parameters: FOV 400×400mm2, TE/TR/FA 1.51ms/4.75ms/35° and pixel size 1.25×1.25mm2. In terms of ST, two values were tested: 6mm and 10mm where SG was adapted to get the basal, median and apical slices according to the subjects’ anatomy (typically 18-25mm SG).
Results
I.A) Unsurprisingly, higher SNR (Fig.1.A) was obtained with greater slice thickness and lower BW. SNR varied faster with ST ([36-130] Fig.1.A) and SG variation ([6-107] Fig.1.B) than with readout BW.
I.B) The results of an SMS3-bSSFP cardiac acquisition on a healthy volunteer are shown in Fig.2. Multiband images were successfully reconstructed. Banding artefacts remained minimal (Fig.2, first row) and the images retained high SNR (Fig.2, second row). There was 64% loss of SNR between non-SMS and SMS images over the 6 volunteers (SNR [non-SMS] = 175±37 and SNR [SMS] = 63±15).
II.A) T1 maps generated from non-SMS and SMS3 MOLLI images with different slice thickness and gap between slices are shown in Fig.3. T1 values from all acquisitions (Fig.3: 6mm-400%gap, 8mm-300% gap and 10mm-250% gap) were in line with the calibrated gold-standard T1 values (Fig.3, top left & bottom left). T1 quantification uncertainty (SD/mean) was doubled when comparing non-SMS T1 maps and SMS T1 maps (non-SMS: 1.5% uncertainty; SMS: 3.9% uncertainty) but remained very tolerable.
II.B) T1 maps in Fig.4 show comparable T1 quantification between the regular single slice acquisition and the SMS3 technique on healthy volunteers. At in-vivo SNR levels, T1 quantification uncertainty values were equivalent between SMS and non-SMS T1 maps (Non-SMS: 15.0% in the myocardium and 9.6% in the blood. SMS: 15.1% in the myocardium and 10.8% in the blood).
Discussion
The sensitivity of SMS3 blipped-CAIPIRINHA-bSSFP was evaluated in terms of SNR to slice gap, pixel bandwidth, slice thickness and robustness of T1 quantification. Eventually, priority is to increase ST and SG within the boundaries of cardiac dimensions, while BW remains low without compromising bSSFP banding artefacts and acquisition-time window. For cardiac SMS bSSFP imaging, despite noise amplification and few remaining SMS-aliasing artefacts, these initial results are very promising. Nevertheless, because intense fat signal appears difficult to unalias properly using the current SMS algorithm, further work considering fat saturation is needed. Additionally, post-contrast investigations using SMS-T1 mapping for shorter T1 values are warranted.Conclusion
The proposed blipped-CAIPI MOLLI T1 mapping sequence provides T1 quantification over three levels of the heart (base, mid and apex) with reliable and accurate values in line with those obtained with a single slice acquisition.Acknowledgements
This work was performed by a laboratory member of France Life Imaging network (grant ANR-11-INBS-0006),on the platform 7T-AMI, a French “Investissements d’Avenir” programme”(grant ANR-11-EQPX-0001).
The authors would like to thank Lauriane Pini and Claire Costes for the help with the MRI examinations.
References
1. Scheffler, K. & Lehnhardt, S. Principles and applications of balanced SSFP techniques. Eur. Radiol.13, 2409–2418 (2003).
2. Setsompop, K. et al.Blipped-controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g-factor penalty. Magn. Reson. Med.67, 1210–1224 (2012).
3. Duerk, J., Griswold, M. & Dara, K. Multi-slice blipped TRUEFISP-CAIPIRINHA. (2012).
4. Weingärtner, S. et al.Simultaneous multislice imaging for native myocardial T 1mapping: Improved spatial coverage in a single breath-hold: Multislice Imaging for Myocardial T 1Mapping.Magn. Reson. Med.78, 462–471 (2017).
5. Cauley, S. F., Polimeni, J. R., Bhat, H., Wald, L. L. & Setsompop, K. Interslice leakage artifact reduction technique for simultaneous multislice acquisitions: Interslice Leakage Artifact Reduction Technique. Magn. Reson. Med.72, 93–102 (2014).
6. Hansen, M. S. & Sørensen, T. S. Gadgetron: An open source framework for medical image reconstruction: Gadgetron. Magn. Reson. Med.69, 1768–1776 (2013).
Figures