2014
Myocardial T1 mapping with Shortened Acquisition Window using a two-layer Sparsifying Transform1Shenzhen Institutes of Advanced Technology, Chinese Academy of Sciences, Shenzhen, China, 2Department of Medicine (Cardiovascular Division), Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, United States
Synopsis
Long acquisition window in myocardial T1 mapping degrades the image quality. Physiological motion induced fluctuations along the parametric direction corrupt the similarity among T1-weighted images and adversely impact the performance of the compressed sensing-based methods. In this study, we propose a two-layer sparsifying transform (MO2) combined with motion correction to shorten the acquisition window of myocardial T1 mapping. Results showed that the proposed method enabled higher acceleration factor. The resulting shorter acquisition window and fewer RF saturation pulses increased the accuracy of the native T1 measurement.
Introduction
Myocardial T1 mapping allows non-invasive assessment of diffuse myocardial fibrosis [1]. It acquires T1-weighted images at a quiescent period of the cardiac motion in mid-diastole or systole. Long acquisition window for each image degrades the image quality, especially in applications with fast heart rates. Parallel imaging is used for accelerating data acquisition but the acceleration rate is only limited to 2. Compressed sensing (CS) methods with single sparsifying transform, i.e. fixed transform or dictionary learning, have been applied for fast myocardial T1 mapping [2,3]. However, physiological motion induced fluctuations along the parametric direction corrupt the similarity among T1-weighted images and adversely impact the performance of the CS-based method. Also, previous studies shown that the combination of fixed and adaptive transform could further promote the sparsity of the signal and the reconstruction quality compared with single transform [4]. In this study, we propose a two-layer sparsifying transform (MO2) combined with motion correction for fast myocardial T1 mapping. It reduces the adverse impact of physiological motion on reconstruction and improves the reconstructed image quality.Methods
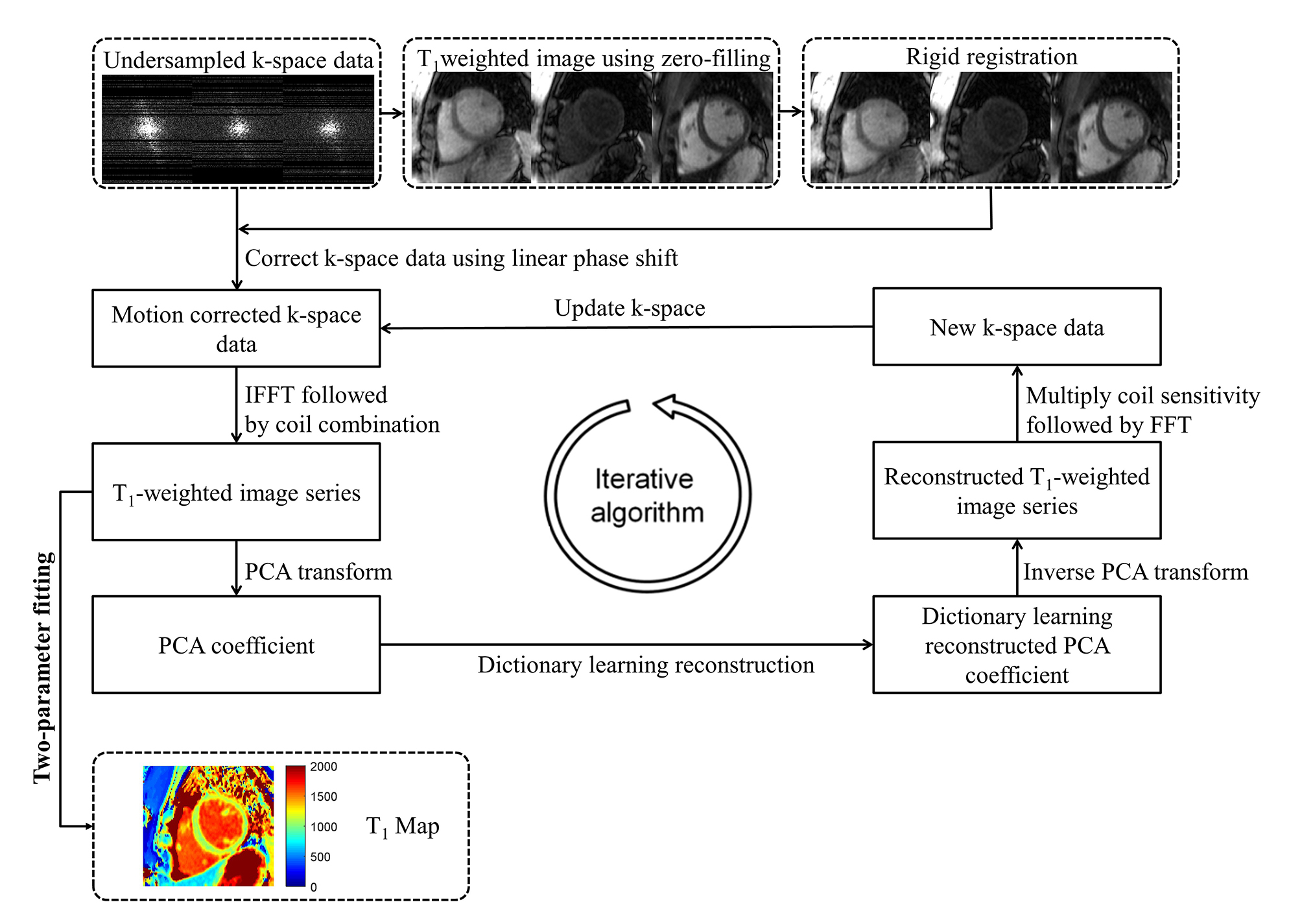
The reconstruction step are summarized in Figure 1. First, T1-weighted images reconstructed using zero filling method are used for rigid registration. The estimated global translational motion is used for k-space data correction using Fourier shift theorem. The corrected k-space data are reconstructed using a two-layer sparsifying transform. Specifically, principal component analysis (PCA) is applied along parametric direction and then dictionary learning is used to reconstruct the sparse PCA coefficients. The T1-weighted images are obtained by transforming the resulting PCA coefficients with inverse PCA transform. The reconstruction problem can be formulated as
$$minimize_{I_p,\alpha_n}\sum_n||D\alpha_n-R_n(B[I_1,...,I_{N_p}])||_2^2+\upsilon\sum_{c,p}||k_{c,p}-F_pS_cI_p||_2^2$$
$$subject\ \ to\ \forall{n}, ||\alpha_0||_0\leq{T_0}$$
where Ip is the p-th vectorized T1-weighted image to be reconstructed, with p = 1, …, Np. Np is the total frame number. Fp is the undersampled Fourier operator. Sc is the c-th coil sensitivity and kc,p is the undersampled k-space data.$$$B=\left\{\overrightarrow{b_1},\overrightarrow{b_2},...,\overrightarrow{b_L}\right\}$$$is the matrix of the PC basis, which is generated using a training data set from T1-weighted images with the singular value decomposition algorithm. Rn represents the operator that extracts the PC coefficients at the same spatial location. D is the patch based dictionary. αn is the sparse representation of patch n with respect to D. T0 is the required sparsity level. ν is the regularization parameter.
Evaluation:
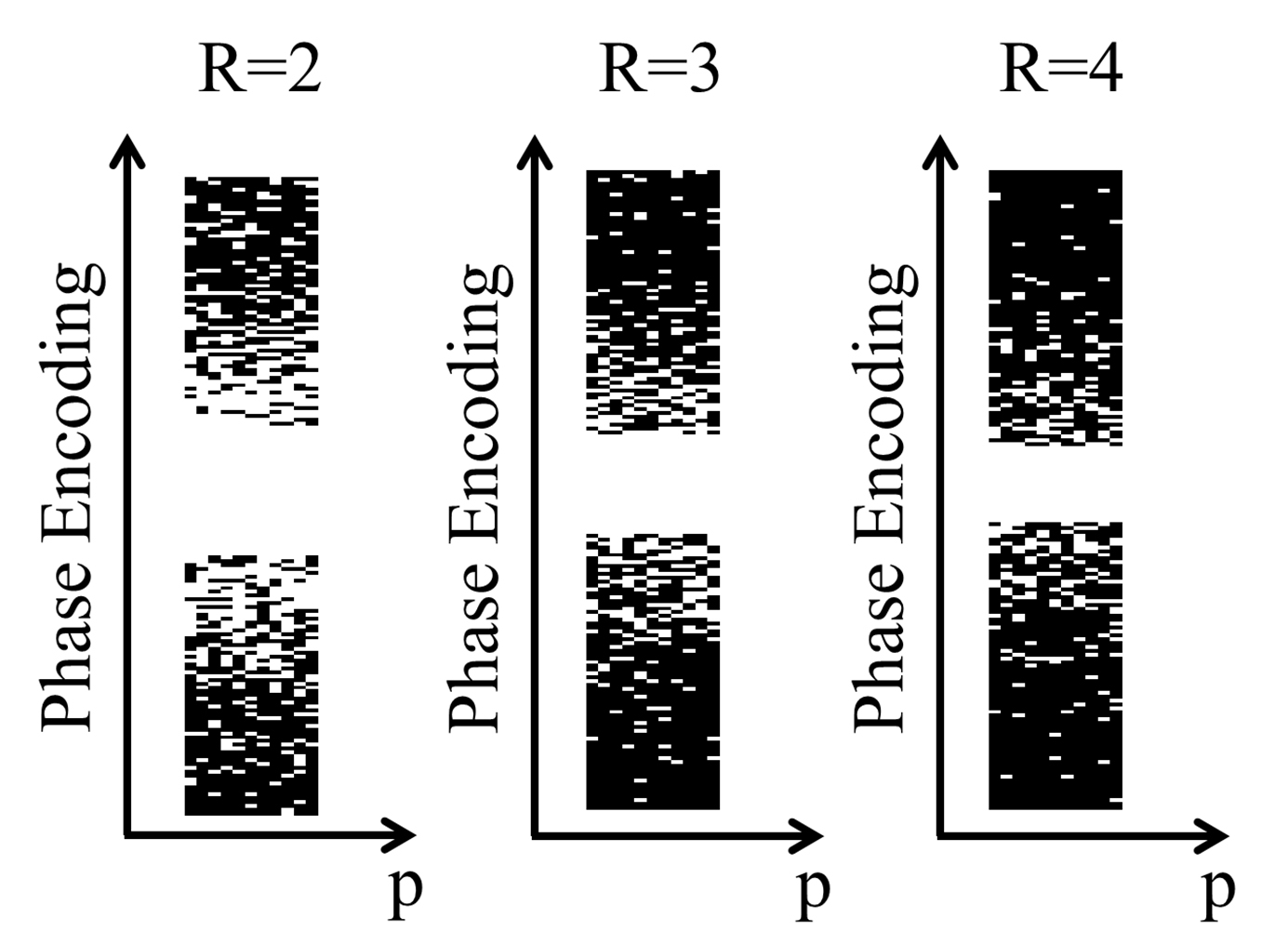
All MR data were acquired on a 1.5 T Philips Achieva (Philips Healthcare, Best, The Netherlands) system with a 32-channel cardiac coil. A random undersampled k-space data acquisition scheme at R=2, 3, and 4 (Figure 2) was implemented for slice-interleaved myocardial T1 mapping sequence (STONE) [5] to allow prospectively randomly undersampling data. T1MES Phantom [6] were scanned with the above acquisition scheme to assess the accuracy and precision of T1 measurements related to the reconstruction method. Imaging parameters were: bSSFP readout with TR/TE/flip angle=3.12ms/1.56ms/70˚, field-of-view=240×228mm2, matrix size=176×167, and simulated ECG of 60 bpm. Reference T1 values of the phantom were measured using an inversion recovery spin echo sequence. For in-vivo experiments, three healthy volunteers (two females, 24±3 years old) were recruited for this study (IRB proved, written informed consents obtained). In each subject, we acquired 6 datasets using prospective undersampling at R=2 through 4 with both random and uniform undersampling masks using STONE sequence. Imaging parameters were the same as in phantom study except TR/TE=2.8ms/1.4ms and FOV=360×342mm2. The proposed method was used to reconstruct T1-weighted images with random undersampling masks and SENSE was used for uniform undersampling reconstruction. All T1 maps were calculated using a two-parameter model from the T1-weighted images.
Results
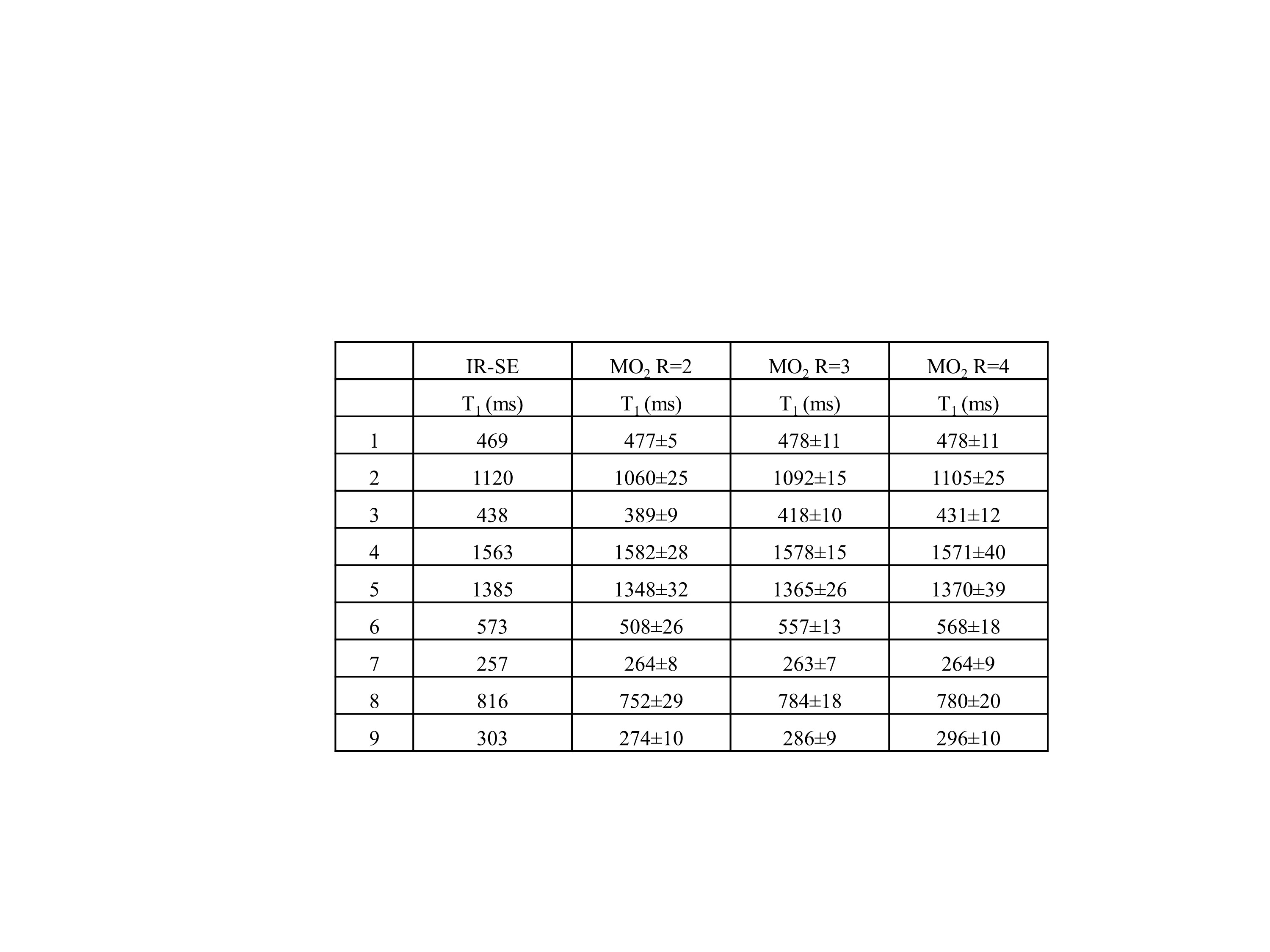
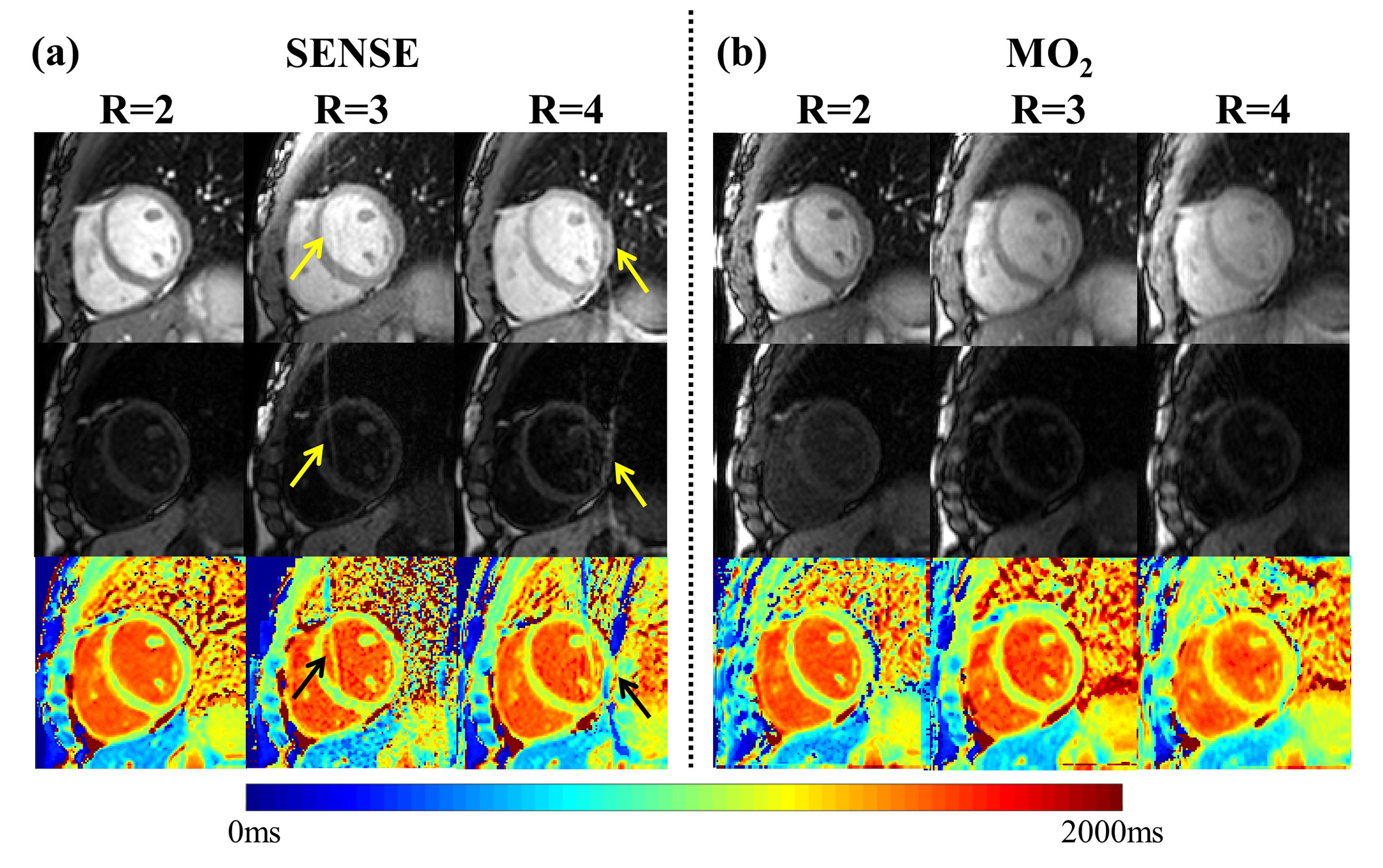
In phantom studies, the accuracy of the T1 measurement (-30±33ms, -11±17ms, and -7±14 ms for R=2 to 4) improved with increasing reduction factors compared with the gold standard, i.e., IR-SE T1 values (Table 1). For in-vivo experiments, all images were reconstructed with MO2 successfully. Figure 3 shows representative results of a healthy volunteer at reduction factor of 2, 3, and 4 using MO2 and SENSE. Aliasing artifacts are observed in T1-weighted images (yellow arrows) and T1 maps (black arrows) with SENSE at reduction factors greater than 2. The global T1 of MO2 were 1051±52ms, 1093±35ms, and 1093±35ms for R = 2 through 4, respectively. In-vivo studies show elevated myocardial T1 values (i.e. improved accuracy) with a shorter acquisition window.Conclusion
We combine a two-layer sparsifying transform and motion correction for fast myocardial T1 mapping. The resulting higher acceleration factor enables a shorter acquisition window and fewer RF saturation pulses, thereby increasing the accuracy of the native T1 measurement.Acknowledgements
No acknowledgement found.References
- Messroghli DR, Moon JC, Ferreira VM, Grosse-Wortmann L, He T, Kellman P, Mascherbauer J, Nezafat R, Salerno M, Schelbert EB, Taylor AJ, Thompson R, Ugander M, van Heeswijk RB, Friedrich MG. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 2017;19(1):75.
- Kang J JJ, Tarokh V, Nezafat R. Dictionary-based Reconstruction for Free-Breathing Myocardial T1 Mapping. 2017; Honolulu,Hi, USA. In Proceedings 23th Scientific Meeting, International Society of Magnetic Resonance in Medicine (ISMRM). p 545.
- Li W, Griswold M, Yu X. Fast cardiac T1 mapping in mice using a model-based compressed sensing method. Magn Reson Med 2012;68(4):1127-1134.
- Zhu Y, Zhang Q, Liu Q, Wang YX, Liu X, Zheng H, Liang D, Yuan J. PANDA-T1rho: Integrating principal component analysis and dictionary learning for fast T1ρ mapping. Magn Reson Med 2015;73(1):263-272.
- Weingärtner S, Roujol S, Akçakaya M, Basha TA, Nezafat R. Free‐breathing multislice native myocardial T1 mapping using the slice‐interleaved T1 (STONE) sequence. Magn Reson Med 2015;74(1):115-124.
- Captur G, Gatehouse P, Keenan KE, Heslinga FG, Bruehl R, Prothmann M, Graves MJ, Eames RJ, Torlasco C, Benedetti G. A medical device-grade T1 and ECV phantom for global T1 mapping quality assurance—the T1 Mapping and ECV Standardization in cardiovascular magnetic resonance (T1MES) program. J Cardiovasc Magn Reson 2016;18(1):58.
Figures