2013
Comparison of cardiac function, morphology and tissue characteristics between two subtypes of primary aldosteronism: a 3 Tesla MR studySatoshi Higuchi1, Hideki Ota1, Kazumasa Seiji1, Yuta Tezuka2, Ryo Morimoto2, Tatsuya Nishii3, Tetsuya Fukuda3, and Kei Takase1
1Diagnostic Radiology, Tohoku university hospital, Sendai, Japan, 2Endocrinology, Tohoku university hospital, Sendai, Japan, 3Radiology, National cerebral and cardiovascular center, Suita, Japan
Synopsis
The purpose of this study is to compare cardiac morphology, function and tissue characteristics between patients with two subtypes of primary aldosteronism (PA), aldosterone-producing adenoma (APA) and bilateral hyperaldosteronism (BHA). One-hundred-and-forty-three consecutive PA patients underwent 3T MR examinations including cine, late gadolinium enhancement and pre- and post-contrast T1 mapping. APA group demonstrated higher myocardial native T1 and left-ventricular end-diastolic volume index than BHA after controlling for patients’ demographic data. The results indicate that APA group, with higher hormonal activity than BHA, may be suffered from LV volume overload and myocardial fibrosis or edema as compared with BHA group.
Introduction
Primary Aldosteronism (PA) is one of the most frequent forms of secondary hypertension. The excess aldosterone has been associated with various cardiovascular damages (1); it has increased risks of cardiovascular events relative to patients with essential hypertension, resulting in increased cardiovascular mortality (2). Two most common causes of PA are unilateral aldosterone-producing adenomas (APAs) and bilateral hyperaldosteronism (BHA). APAs often secrete higher amounts of adrenocortical hormone compared to adrenals of BAH patients. In echocardiographic assessment, left ventricular (LV) end-diastolic and end-systolic diameters, and LV mass were greater in APA group than BHA group (3). However, there has been little reports comparing cardiac characteristics among subtypes of PA. The purpose of this study is to compare cardiac morphology, function and tissue characteristics between patients with APAs and BHA using a 3T MR scanner.Methods
We included 143 consecutive patients with PA and no history of heart disease or severe renal dysfunction (mean age, 52±12 years, male, 75). All patients were diagnosed by endocrinologists from September 2015 to May 2018 according to a Japanese guideline. (4) All patients underwent cardiac MR examination and adrenal venous sampling to determine the laterality of the PA lesion. Scan protocols included cine, late gadolinium enhancement (LGE) and pre- and post-contrast T1 mapping by modified Look-Locker inversion recovery. We evaluated the presence of LGE, native T1 values and extracellular volume (ECV) and the following LV volumetric parameters: end-diastolic and end-systolic septum wall thickness, ejection fraction, end-diastolic, end-systolic and stroke volume index (EDVI, ESVI and SI), cardiac index (CI) and LV mass index. Regions of interests for evaluation of native T1 and ECV were placed on the mid-wall of the basal septum. Patients' demographic characteristics were collected; including sex, age, body mass index, family history of essential hypertension, medical history of diabetes mellitus, smoking history, the number of antihypertensive drugs, home systolic blood pressure and disease duration which is the interval from appearance of subjective symptoms or notice of hypertension to the diagnosis. We also collected the level of plasma aldosterone concentration (PAC). Fisher’s exact test was used for dichotomous data, and variables between the two groups with APAs and BHA were compared using Student t-tests or Mann-Whitney’s U tests. Associations among MR parameters, patients' demographic data and subtypes of PA were examined using multivariate logistic regression models. Spearman’s rank correlation coefficient was used to evaluate correlations between two parameters. P < 0.05 was considered statistically significant.Results
Subtypes of PA were diagnosed as APA in 70 (male, 45) and BHA in 73 (male, 30) patients by adrenal venous sampling. In the demographic data, the male proportion (APA vs. BHA = 64% vs. 41%, p<0.01), disease duration (8.5[4-15] vs. 5[2-10.5] years, p=0.03) and the number of antihypertensive drugs (2[1-2] vs. 1[1-2], p<0.01) were significantly larger in APA group than BHA group. After controlling for these parameters as confounders, APA group showed significantly higher native T1 (adjusted odds ratio [aOR] =1.01 [95% CI: 1.000-1.019], p=0.038), EDVI (aOR=1.06 [95% CI: 1.030-1.096], p<0.01), ESVI (aOR =1.06 [95% CI: 1.017-1.113], p<0.01), SI (aOR=1.07, [95% CI: 1.020-1.121], p<0.01), CI (aOR=1.001 [95% CI: 1.000-1.001], p<0.01) than BHA group. APA group showed significantly higher PAC levels than the other (log PAC; 1.7 ± 0.3 vs. 1.3 ± 0.1, p<0.01). Log PAC have positive correlations with EDVI (R=0.28 p<0.01), ESVI (R=0.26 p<0.01) and SI (R=0.18 p=0.03).Discussion
Aldosterone is the main mineralocorticoid hormone which promotes water retention. Our results indicated the influence of acting aldosterone was severer on LV volumetric parameters in APA group with higher aldosterone activity than BHA group, suggesting APA patients are exposed to increased risk of LV volume overload. Moreover, we revealed these volumetric parameters have positive correlations with PAC. Past MR study showed patients with PA demonstrated a significant increase in the frequency of LV hypertrophy and LGE than patients with essential hypertension (5,6). In this study, LV mass, ECV and presence of LGE did not show the significant difference between the two groups; however, elevated native T1 values in APA group may indicate they have mild myocardial fibrosis or edema. Follow-up MR studies are needed to reveal whether resection of the functioning adrenal tumors improves the MR findings in APA group. Moreover, clinical follow-up is also needed to determine the long-term clinical significance of these results.Conclusion
After controlling for patients’ demographic data, APA with higher hormonal activity than BHA demonstrated higher LV volume parameters and myocardial native T1. Among PA patients, APA group may have an increase in the frequency of LV volume overload and mild myocardial fibrosis or edema than BHA group.Acknowledgements
No acknowledgement found.References
- Rossi G-P, Sechi LA, Giacchetti G, Ronconi V, Strazzullo P, Funder JW. Primary aldosteronism: cardiovascular, renal and metabolic implications. Trends Endocrinol Metab. 2008 Apr;19(3):88–90.
- Monticone S, D’Ascenzo F, Moretti C, Williams TA, Veglio F, Gaita F, et al. Cardiovascular events and target organ damage in primary aldosteronism compared with essential hypertension: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2018 Jan 1;6(1):41–50.
- Hidaka T, Shiwa T, Fujii Y, Nishioka K, Utsunomiya H, Ishibashi K, et al. Impact of aldosterone-producing adenoma on cardiac structures in echocardiography. J Echocardiogr. 2013 Dec;11(4):123–9.
- Nishikawa T, Omura M, Satoh F, Shibata H, Takahashi K, Tamura N, et al. Guidelines for the diagnosis and treatment of primary aldosteronism -The Japan Endocrine Society 2009-. Endocr J. 2011;58(9):711–21.
- Freel EM, Mark PB, Weir RAP, McQuarrie EP, Allan K, Dargie HJ, et al. Demonstration of Blood Pressure-Independent Noninfarct Myocardial Fibrosis in Primary Aldosteronism: A Cardiac Magnetic Resonance Imaging Study. Circ Cardiovasc Imaging. 2012 Nov 1;5(6):740–7.
- Gaddam K, Corros C, Pimenta E, Ahmed M, Denney T, Aban I, et al. Rapid Reversal of Left Ventricular Hypertrophy and Intracardiac Volume Overload in Patients With Resistant Hypertension and Hyperaldosteronism. Hypertension. 2010 May 1
Figures
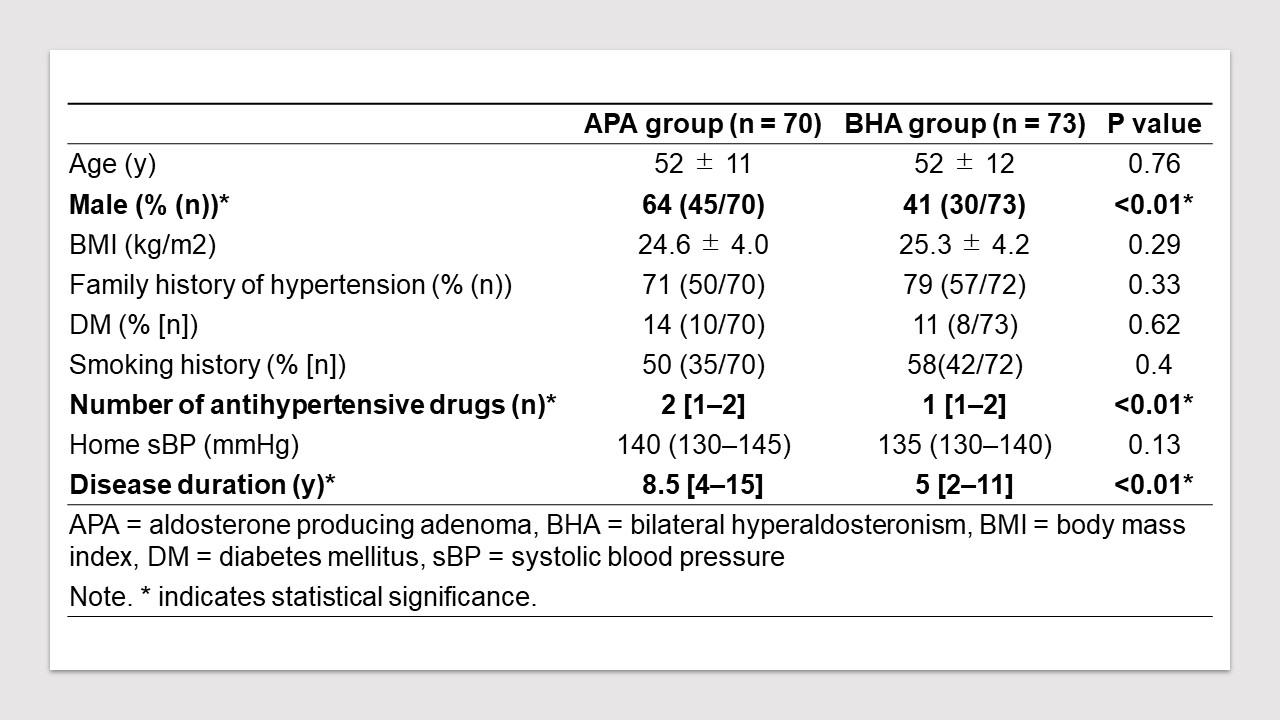
Table
1: Patient demographic characteristics.
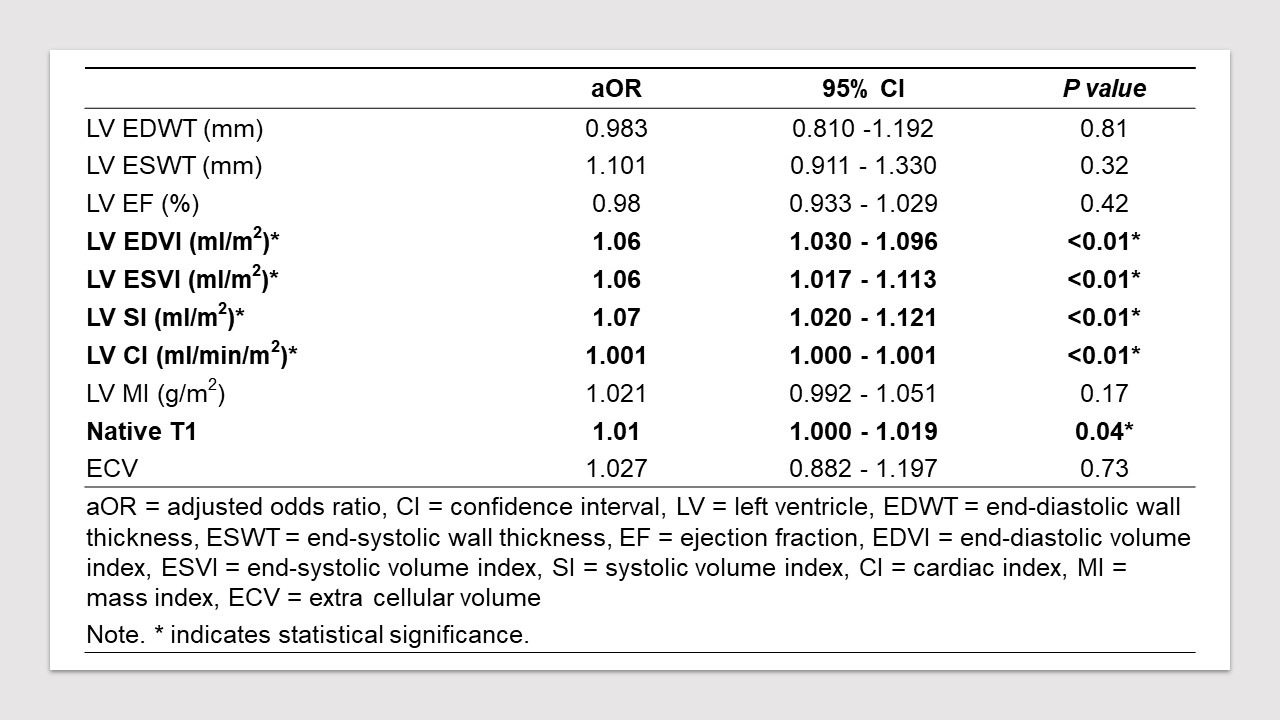
Table
2: Results of multivariate logistic
regression analysis for each MR parameters after controlling for age, sex, number
of antihypertensive drugs and disease duration.
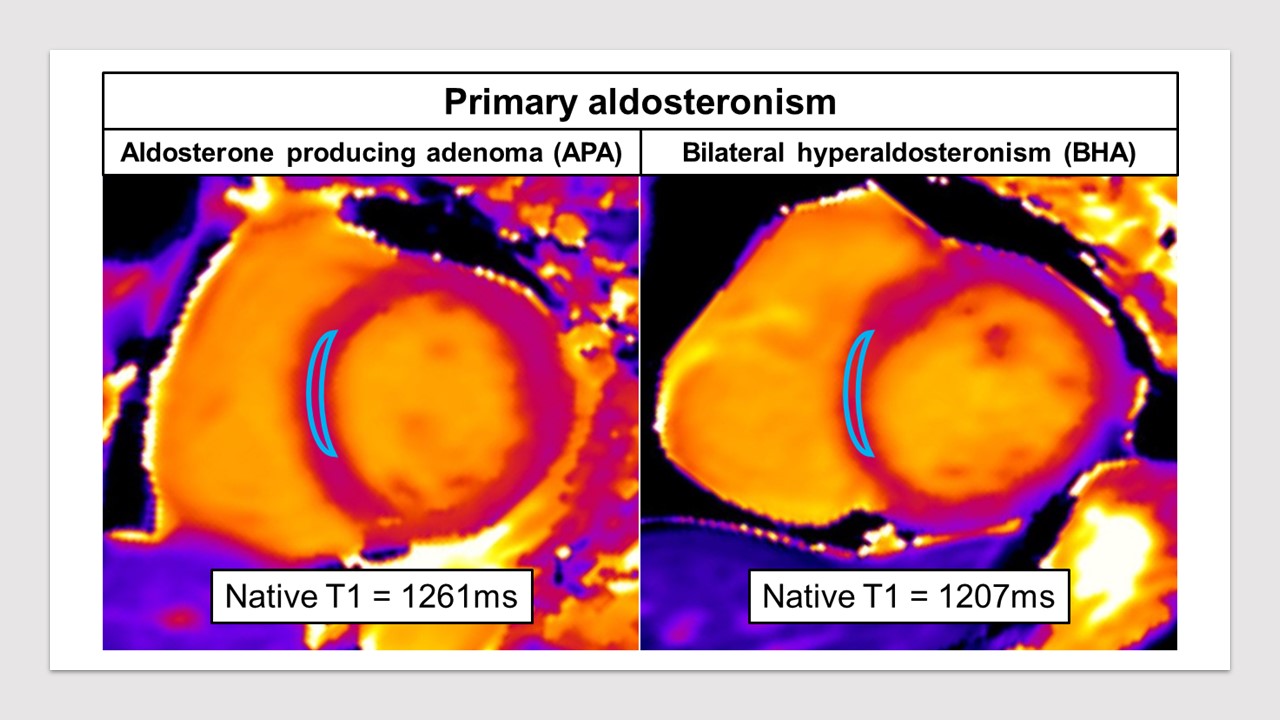
Figure 1: Regions of interests for
evaluation of native T1 and ECV were placed on the mid-wall of basal septum. The
representative cases were shown in aldosterone producing adenoma and bilateral
hyperaldosteronism group.
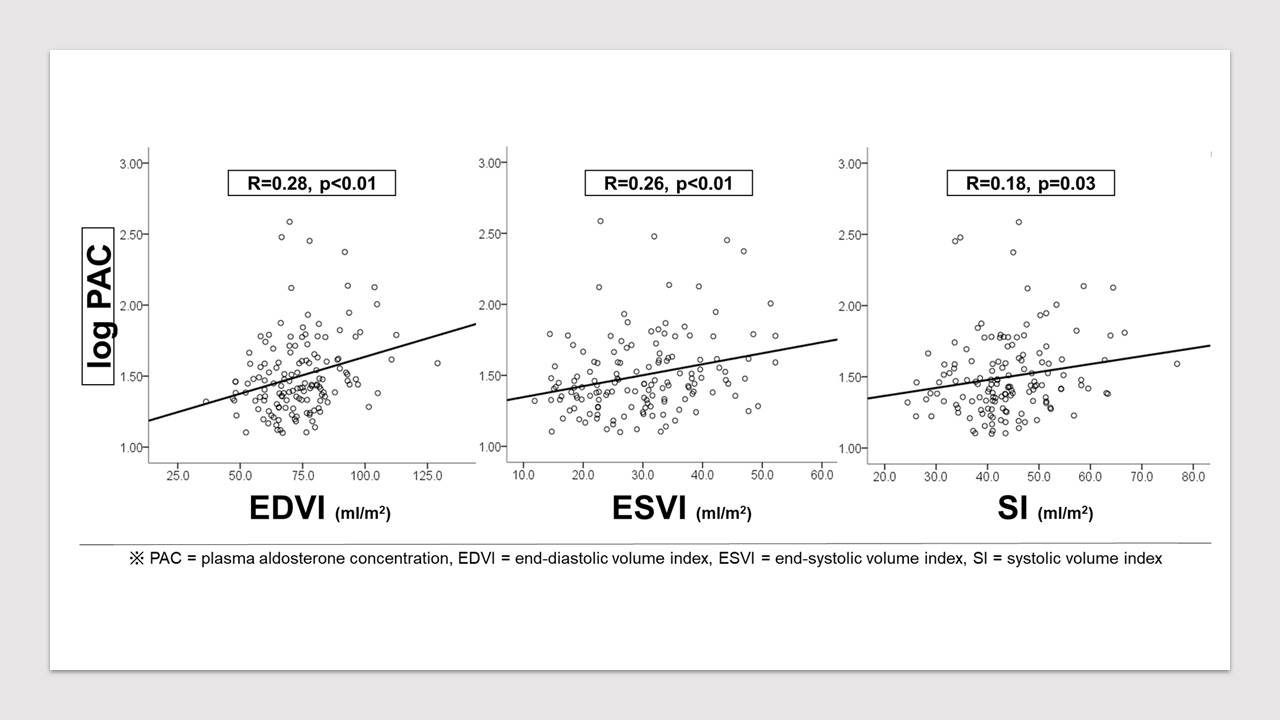
Figure 2: The positive correlation
between log PAC and left ventricle volumetric parameters (EDVI,ESVI,SI).