2006
Impact of a ten-year national Italian networking on cardiac complications in patients with thalassemia major1Fondazione G. Monasterio CNR-Regione Toscana, Pisa, Italy, 2Ospedale del Delta, Lagosanto (FE), Italy, 3Azienda Ospedaliero-Universitaria Ospedali Riuniti "Umberto I-Lancisi-Salesi", Ancona, Italy, 4Presidio Ospedaliero “Giovanni Paolo II”, Lamezia Terme (CZ), Italy, 5Azienda Ospedaliera "Garibaldi", Presidio Ospedaliero Nesima, Catania, Italy, 6Policlinico "Paolo Giaccone", Palermo, Italy, 7Fondazione di Ricerca e Cura "Giovanni Paolo II", Campobasso, Italy, 8Presidio Ospedaliero “Umberto I”, Siracusa, Italy, 9Azienda Ospedaliera di Legnago, Legnago (VR), Italy
Synopsis
Over a period of 10 years, the continuous monitoring of cardiac iron levels and a tailored chelation therapy allowed a reduction of myocardial iron overload (MIO) in the 70% of patients with thalassemia major (TM) enrolled in the MIOT (Myocardial Iron Overload in Thalassemia) Network. A consequent improvement of cardiac function and a reduction of heart failure were detected. So, a national networking was effective in improving the care and reducing cardiac outcomes of TM patients.
Introduction
The MIOT (Myocardial Iron Overload in Thalassemia) Network was a network of thalassemia and CMR centers built in 2006 in order to assure homogeneous and standardized cardiac iron overload assessment for a significant number of patients1.
We describe the impact of this ten-year Network on cardiac iron and complications in patients with thalassemia major (TM).
Methods
We considered 1401 TM patients who performed an end-of-study CMR.
Myocardial iron overload (MIO) was quantified by the multislice multiecho T2* technique2. Biventricular function was quantified by cine images3.
Results
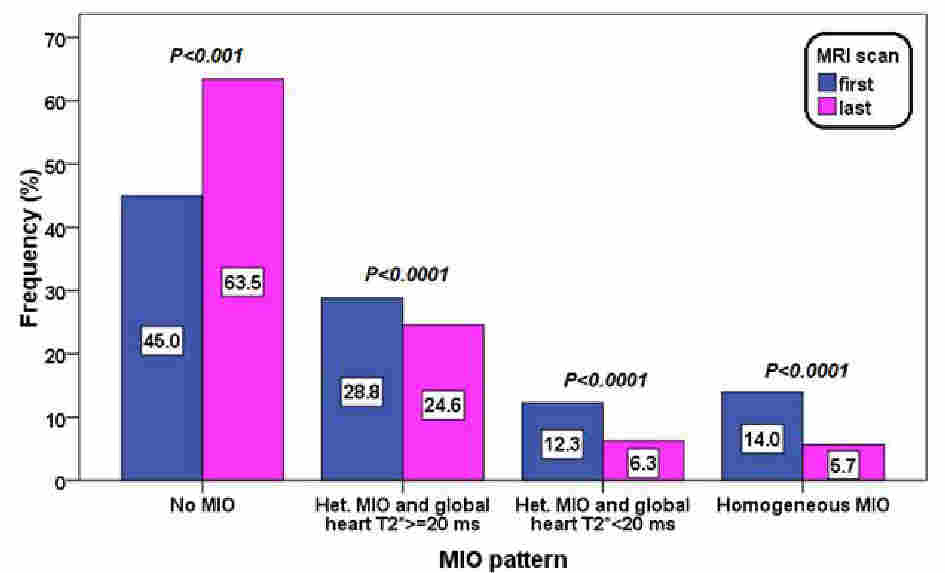
At the last CMR significantly higher global heart T2* values (35.5±10.7 ms vs 29.2±12.0 ms; P<0.0001) and a significant lower number of patients with global heart T2*<20 ms (26.3% vs 12.0%; P<0.0001) were detected. Four patterns of MIO were identified: no MIO (all segments with T2*≥20 ms), heterogeneous MIO and global heart T2*≥20 ms, heterogeneous MIO and global heart T2*<20 ms, and homogeneous MIO (all T2*<20 ms). Figure 1 shows the frequency of the 4 patterns at both scans. At the last CMR a significant higher frequency of patients with no MIO and a significant lower frequency for the other three patterns indicating MIO were detected. An improvement in MIO, that is a transition to a better risk class, was detected in the 68.4% of patients with at least one pathologic segment at the baseline.
In patients with global heart T2*<20 ms a significant increase in left ventricular ejection fraction (EF) (difference: 3.2±8.5 %, P<0.0001) as well as in right ventricular EF (difference: 1.2±8.9 %, P=0.002) were detected.
Based on CMR results the 75% of the patients changed the chelation therapy. At the last CMR the percentage of patients with an excellent/good compliance was significantly higher (94.7% vs 92.7%%; P=0.034).
The 13.1% of the patients had a cardiac complication (heart failure, arrhythmias, pulmonary hypertension, myocardial infarction, angina, myo/pericarditis, peripheral vascular disease) before the enrolment in the project. During the study, the frequency of cardiac complications was 7.9 %, significantly lower (P<0.0001). In particular, the frequency of heart failure was significantly lower (5.9% vs 1.7%, P<0.0001).
Conclusions
Over a period of 10 years, the continuous monitoring of cardiac iron levels and a tailored chelation therapy allowed a reduction of MIO in the 70% of patients and a consequent improvement of cardiac function and reduction of heart failure. So, a national networking was effective in improving the care and reducing cardiac outcomes of TM patients.Acknowledgements
No acknowledgement found.References
1. Meloni A, Ramazzotti A, Positano V, et al. Evaluation of a web-based network for reproducible T2* MRI assessment of iron overload in thalassemia. Int J Med Inform 2009;78(8):503-512.
2. Meloni A, Positano V, Pepe A, et al. Preferential patterns of myocardial iron overload by multislice multiecho T*2 CMR in thalassemia major patients. Magn Reson Med 2010;64(1):211-219.
3. Aquaro GD, Camastra G, Monti L, et al. Reference values of cardiac volumes, dimensions, and new functional parameters by MR: A multicenter, multivendor study. J Magn Reson Imaging 2016;45(4):1055-1067.
Figures