1998
Auto-calibrated Simultaneous Multi-Slice Pulse-Wave Velocity Imaging1Physikalisch-Technische Bundesanstalt (PTB), Braunschweig and Berlin, Germany, 2Department of Radiology, Northwestern University, Feinberg School of Medicine, Chicago, IL, United States
Synopsis
Pulse Wave Velocity (PWV) MR imaging is an established technique to derive aortic stiffness. The underlying phase-contrast velocity data is typically acquired during multiple breath-holds within multiple 2D planes placed perpendicularly to the aorta. In this work we investigate the application of an auto-calibrated multiband approach to simultaneously excite and acquire three slices. With this technique all data is obtained in a single breath-hold and without the need of external reference scans. Blood velocities and PWV for different MB acquisitions are compared to results obtained with a singleband approach that excites each slice separately.
Introduction
Pulse Wave Velocity (PWV) MR imaging is an established technique to derive aortic stiffness. PWV can be obtained from phase-contrast velocity measurements with high temporal resolution1 (10-30ms) in multiple 2D slices placed perpendicularly to the aorta. Usually, the slices are acquired sequentially during multiple breath-holds, making the technique susceptible to potential hemodynamic fluctuations between breath-holds, which may affect PWV results. This problem can be avoided by simultaneous multi-slice imaging (SMS)2, also termed "multiband" (MB). MB has been previously applied to PWV imaging to simultaneously acquire two separate slices3 and velocity data was acquired in one breath-hold. Additional calibration scans were obtained separately3, which however may require an additional breath-hold. Here, we apply SMS with two (MB2) and three (MB3) slices for PWV calculation, cutting the ascending (AAo,slice 1), and descending aorta (DAo,slice 2) and in case of MB3 also the common carotid arteries (CA,slice 3). In contrast to ref.3 an auto-calibrated approach is used that derives the calibration data from the MB data itself, thus no external reference data is required. Therefore, as opposed to standard singleband (SB) approaches, the method allows for truly simultaneous imaging within a single breath-hold, eliminating potential errors due to physiological variations.Methods
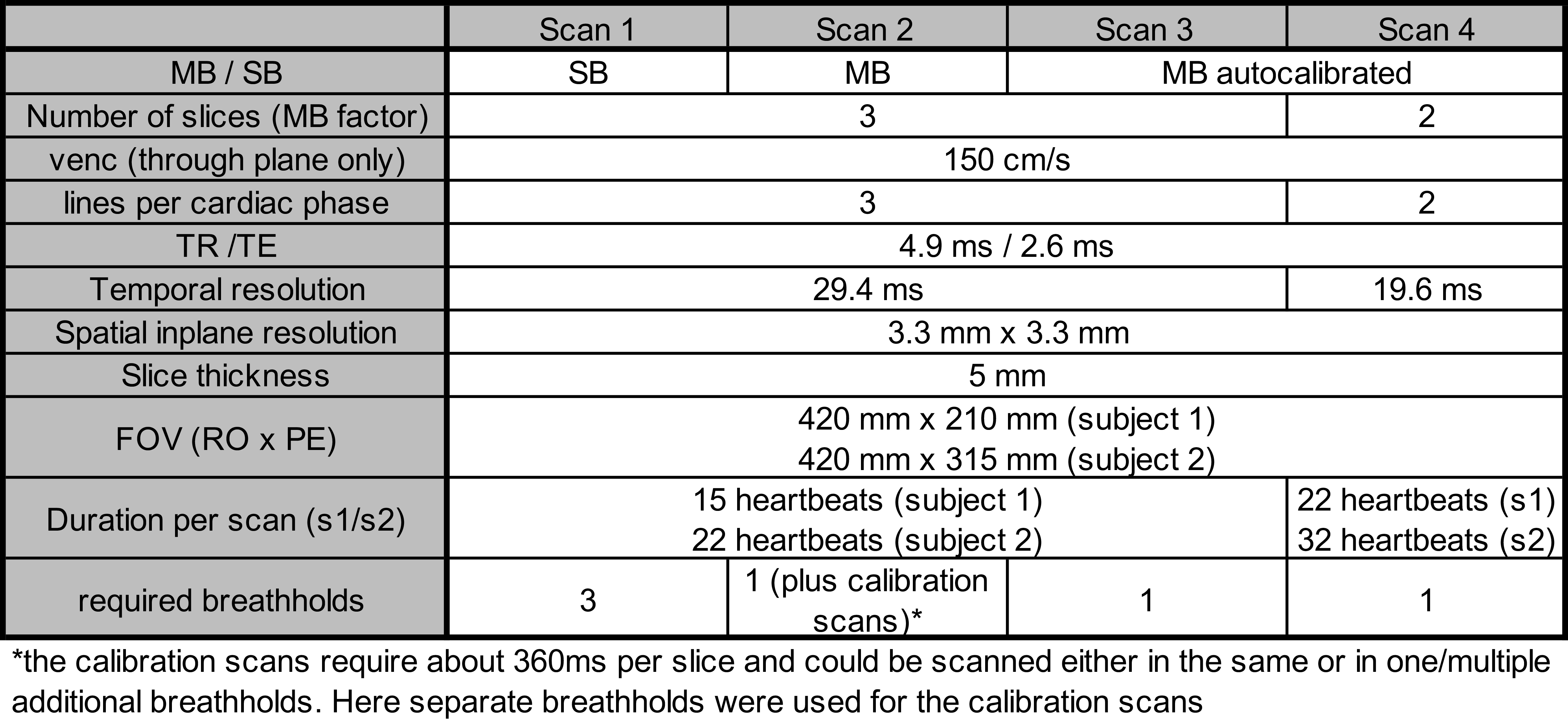
Two healthy subjects (S1:25years, S2:69years) were scanned at 3T (Siemens Verio, Germany) using four phase-contrast velocity acquisitions with parameters listed in Tab.1: an SB acquisition performed sequentially at all three slices (scan 1), two different MB3 acquisitions (scans 2-3) and one MB2 acquisition (scan 4) with higher temporal resolution. Slices were positioned non-equidistantly (Fig.1a). No in-plane acceleration was used resulting in extended breath-holds (22-32sec) performed during inhale. MB pulses were generated by complex summation of sinc-shaped SB pulses. CAIPIRINHA4 was applied for all SMS acquisitions to shift the field-of-view in phase-encoding direction and the slices were separated using a split-slice GRAPPA algorithm5. For scan 2, the CAIPIRINHA phases were constant through time and separate, non-time-resolved gradient-echo calibration scans were obtained in separate breathholds for slice separation6. Scans 3+4 did not need this extra dataset, instead an auto-calibrated MB (MBauto) approach7 was used. Enabled by applying alternating CAIPIRINHA phases through time, the three slices for MB3 were separated using three adjacent cardiac phases. This resulting low-temporal resolution data was used to generate the slice-GRAPPA kernels applied to unalias the MBauto datset at original temporal resolution. Thus, all data was obtained in one breathhold. Scan 4 was identical to scan 3 except that only AAo and DAo were excited (i.e. MB2), but data was acquired at higher temporal resolution (19.6ms; scans1-3:29.4ms). Signal leakage between slices was quantified as in ref.6 by the 99th percentile of the leaking magnitude (L99) and given in percent of the mean SB signal within the aorta. ROIs covering the AAo, DAo and CA were segmented manually and mean velocities over the ROIs were calculated yielding time-resolved velocity curves v(t) for each vessel segment. A Wilcoxon signed rank test was performed to test for statistical differences between the v(t) curves. Curves were linearly interpolated on a sub-millisecond grid and PWV were calculated using cross-correlations and slice distances along the vessel center-line.Results
The animated Fig.2 illustrates reconstructed images of the non-separated (column 1) and slice-separated (columns 2-4) auto-calibrated MB3 dataset. Clean magnitude/phase images without visual artifacts were achieved, which is quantitatively supported by low signal leakage of L99=2.3%. v(t) curves obtained with MB qualitatively agree with those obtained using the SB as shown in Fig.3. Mean v(t) difference between MBauto and SB was <0.5cm/s and not significant. Time-resolved curves of the spatially averaged velocities across AAo and DAo and cross-correlation curves are shown in Fig.4 for the MB2auto dataset. PWVs between AAo and DAo planes for scans 1-4 were 3.1m/s (SB), 3.7m/s (MB3), 3.3m/s (MB3auto), 3.6m/s (MB2auto) for S1 and 7.2m/s (SB), 7.0m/s (MB3), 7.8m/s (MB3auto), 8.0m/s (MB2auto) for S2. PWV between AAo and CA resulted in nominally negative values for SB, MB3 and MB3auto, which can be attributed to differences in pulse shapes and to the temporal resolution of scans 1-3 that is likely not sufficient for such short distances (8.5cm/8.7cm) between AAo and CA.Discussion and Conclusion
This study demonstrates the feasibility of auto-calibrated MB PWV imaging in three slices within one breath-hold. Reasonable PWV values were obtained within the Aorta that agreed between MB2 and MB3 datasets, reflecting normal values in the younger and elevated values in the older subject. Slice 3 was placed in the CA, here, but could also be used as an additional aortic slice to improve robustness of the PWV calculation. Shorter scan times and even higher temporal resolutions are achievable by adding in-plane acceleration. In future, investigations in a larger cohort are planned for statistical analysis.Acknowledgements
No acknowledgement found.References
1Wendland et al. Cardiovasc Diagn Ther. 2014 Apr;4(2):193-206
2Larkman et al. J Magn Reson Imaging. 2001;13(2):313-7
3Jin et al. Proceedings ISMRM 2017:1265
4Breuer et al. Magn Reson Med. 2005 Mar;53(3):684-91
5Cauley et al. Magn Reson Med. 2014 Jul;72(1):93-102
6Schmitter et al. Magn Reson Med. 2017 Mar;77(3):1010-1020
7Ferrazzi et al. Magn Reson Med. 2018 Sep 17. doi: 10.1002/mrm.27460
Figures