1997
Highly-accelerated real-time phase-contrast and cine MRI using radial k-space sampling and compressed sensing for imaging blood flow and function in the left atrium: inter-scan reproducibility analysis1Northwestern University, Chicago, IL, United States
Synopsis
Standard ECG-gated phase-contrast (PC) and cine MRI methods are likely to produce non-diagnostic image quality and/or poor reproducibility in patients with atrial fibrillation due to irregular heart rhythm. One approach to address this problem is to develop highly-accelerated real-time PC and cine MRI acquisitions which are insensitive to arrhythmia. In response, we developed such methods using radial k-space sampling and compressed sensing. In this study, we sought to evaluate the inter-scan reproducibility of highly accelerated real-time PC and cine MRI methods for imaging blood flow and function in the left atrium.
Introduction
Stroke prevention is one of the major therapeutic goals in atrial fibrillation (AF) management1,2. Traditional risk scores such as the CHA2DS2-VASc score have only modest predictive accuracy. One approach to improve accuracy is to measure blood stasis (one of Virchow's triad) using phase-contrast (PC) MRI and/or left atrial (LA) function, including assessment of beat-to-beat variations. Conventional ECG-gated, breath-hold PC and cine MRI methods are likely to produce low diagnostic yield in patients with AF due to arrhythmia. In response, we developed rapid real-time PC MRI3 and cine MRI4 sequences using radial k-space sampling and compressed sensing (CS). The purpose of this study is to evaluate the inter-scan reproducibility of flow metrics and function in the LA obtained with highly-accelerated real-time PC and cine MRI methods in volunteers.Methods
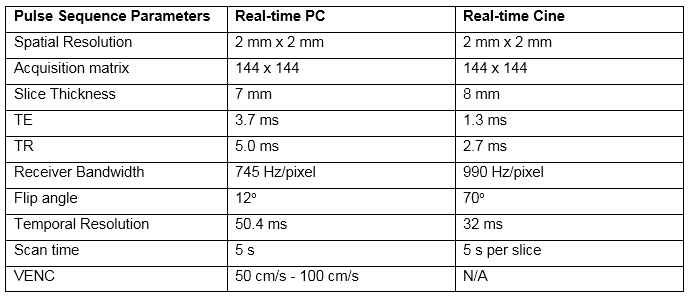
Pulse Sequence & Human Subject: 9 volunteers (6 males, mean age = 60 ± 18 years) in sinus rhythm were scanned twice (1-2 weeks apart) on a 1.5 T scanner (Siemens, AERA). Real-time PC MRI was performed at the inlet of the left atrial appendage (LAA inlet) (venc = 50 cm/s), at the middle of the left atrial appendage (mid LAA) (venc = 50 cm/s), at the middle of the left atrium (mid LA) (venc = 70 cm/s), and just above the mitral valve (above MV) (venc = 100 cm/s). Real-time cine imaging, as previously described4, was performed over the whole heart to measure cardiac functional parameters of the LA and left ventricle (LV). Anatomic landmarks were used to reproduce imaging planes between test and retest. The relevant imaging parameters for PC and cine are summarized in Table 1.
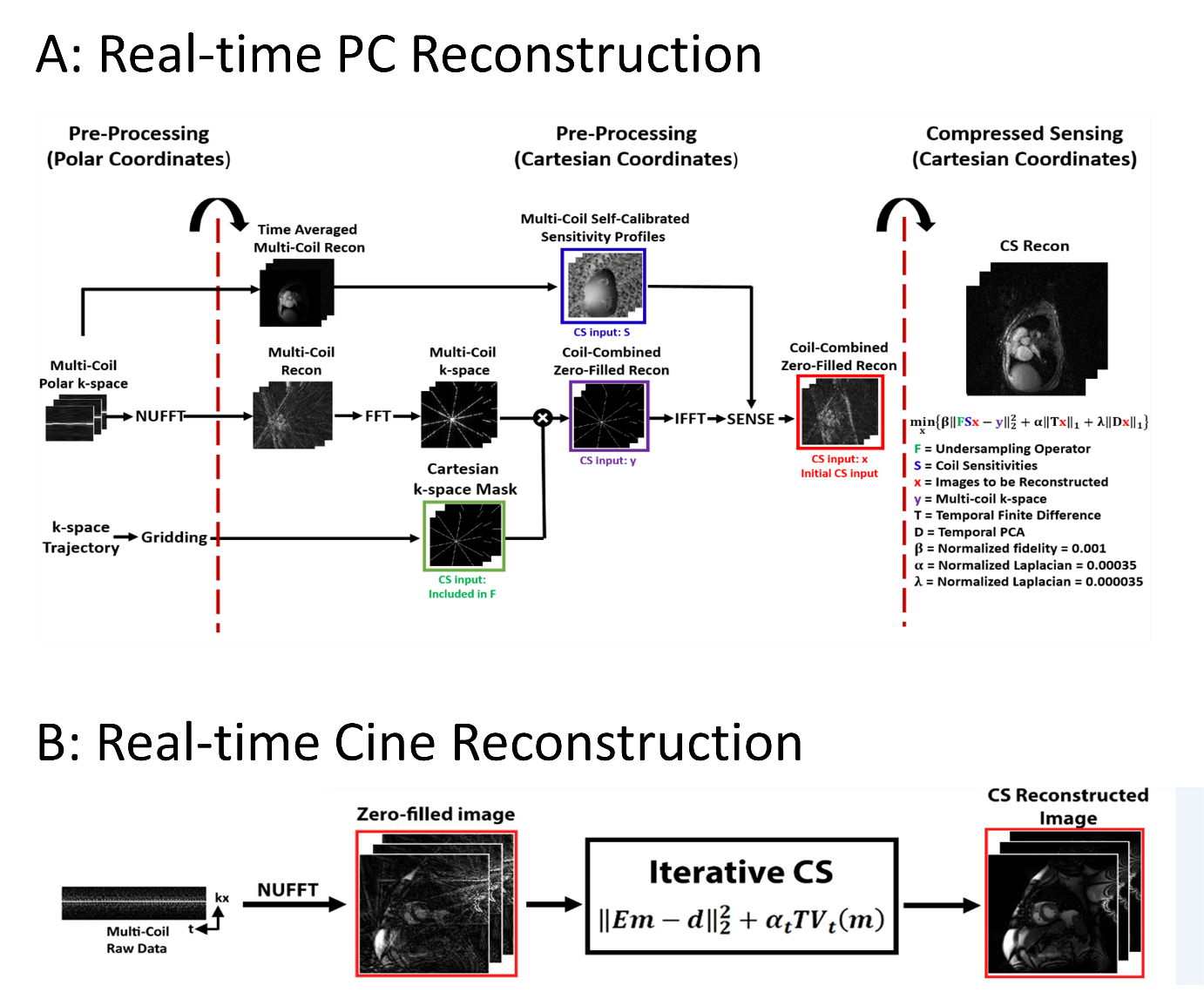
Image Reconstruction: The CS reconstruction was performed off-line as done in previously published methods3,4. For cine imaging, temporal total variation was used as the sparsifying transform, whereas both temporal total variation and temporal principal components were used as two orthogonal sparsifying transforms for the phase contrast imaging (Figure 1). Regularization weights were determined empirically based on visual analysis of training data sets.
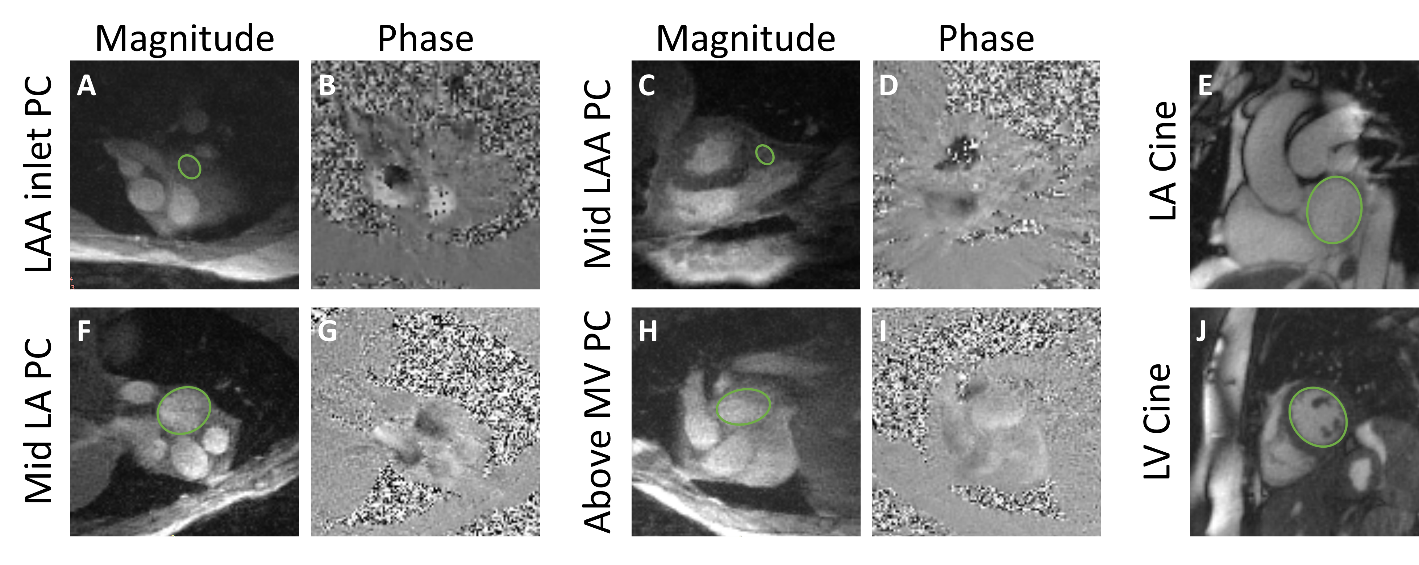
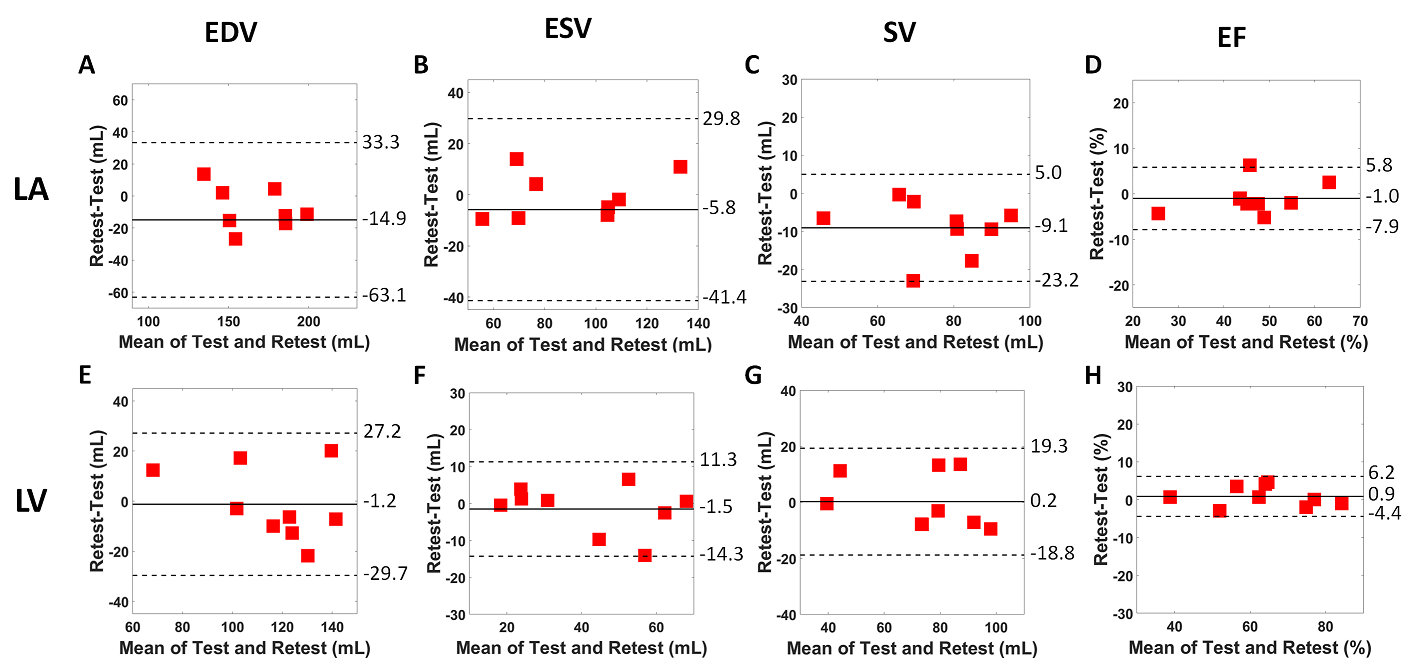
Data Analysis: For PC data, a region of interest was drawn on a workstation equipped with CVI42 (Circle Cardiovascular Imaging Inc.). For cine data, endocardial contours were drawn manually at end diastole and end systole (Figure 2). Peak velocity and cardiac functional parameters (ejection fraction [EF] and volume measurements [end diastolic volume (EDV), end systolic volume (ESV), and stroke volume (SV)]) were computed and compared using Bland Altman analyses.
Results
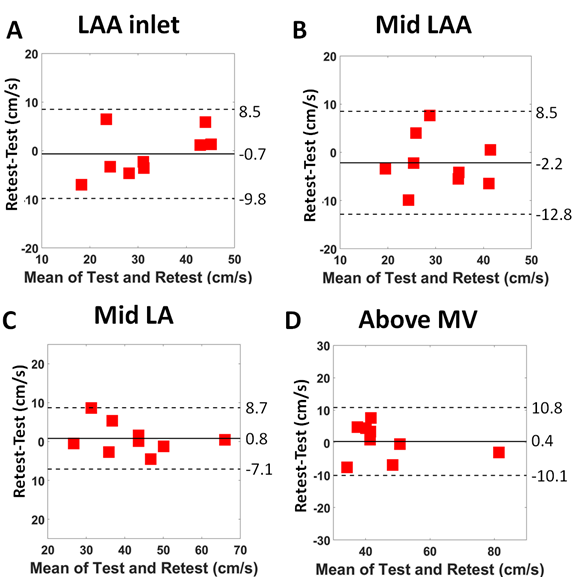
Highly-accelerated real-time PC and cine datasets produced good image quality (Figure 2). Mean peak velocity was 32.0 ± 9.8 cm/s, 30.7 ± 8.0 cm/s, 42.3 ± 11.4 cm/s, and 46.3 ± 13.9 cm/s for the LAA inlet, mid LAA, mid LA, and above MV, respectively. Repeated peak velocity values were strongly correlated (R2 = 0.84 LAA inlet, R2 = 0.61 mid LAA, R2 = 0.90 mid LA, R2 = 0.87 above MV) and in good agreement (maximum mean difference = 2.2 cm/s [7.1% relative to mean]; maximum coefficient of repeatability = 10.7 cm/s [34.8% relative to mean]) (Figure 3). Mean LA EF was 46.4 ± 9.9% and mean LV EF was 63.8 ± 13.5%. EF measurements were highly correlated for both the LA (R2 = 0.90) and LV (R2 = 0.96) and in excellent agreement (LA: mean difference = 1.0% [2.2% relative to mean]; coefficient of repeatability = 6.9% [14.7% relative to mean]; LV: mean difference = 0.9 % [1.4% relative to mean]; coefficient of repeatability = 5.3% [8.3% relative to mean]) (Figure 4). Additionally, LA and LV volume measurements were all in good agreement (Figure 4).Discussion
The proposed real-time PC MRI and cine MRI produced relatively precise maximum velocity results in the LAA inlet, mid LAA, mid LA, and above MV and functional volume parameters for the LA and LV of volunteers in sinus rhythm. Possible sources of variability in data include differences in imaging planes, physiology, and intra-observer variability in data analysis. A future study is warranted to evaluate the reproducibility of these real-time acquisition methods in patients with AF and correlate the resulting metrics to clinical profiles or outcomes.Acknowledgements
This work was supported in part by the following grants: NIH R01HL116895, R01HL138578, R21EB024315, R21AG055954References
1. Fuster V, Ryden LE, Cannom DS et al. 2011 ACCF/AHA/HRS Focused Updates Incorporated Into the ACC/AHA/ESC 2006 Guidelines for the Management of Patients With Atrial Fibrillation A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2006 WRITING COMMITTEE MEMBERS Developed in partnership with the European Society of Cardiology and in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Journal of the American College of Cardiology 2011;57:E101-E198.
2. Lee Park K, Anter E. Atrial Fibrillation and Heart Failure: A Review of the Intersection of Two Cardiac Epidemics. J Atr Fibrillation 2013;6:751.
3. Hassan Haji-valizadeh BDA, Roberto Sarnari, Matthew Barrett, Daniel Kim. Rapid, Real-Time, Phase-Contrast MRI using Compressed Sensing Reconstruction with Split High- and Low-Spatial Frequency Fidelity Terms: A Feasibility Study in Pediatric Patients Society of Cardiac Magnetic Resonance, 2018.
4. Haji-Valizadeh H, Rahsepar AA, Collins JD et al. Validation of highly accelerated real-time cardiac cine MRI with radial k-space sampling and compressed sensing in patients at 1.5T and 3T. Magn Reson Med 2018;79:2745-2751.
Figures