1995
Highly accelerated 4D flow with compressed sensing for efficient evaluation of whole-heart hemodynamics1Radiology, Northwestern University, Chicago, IL, United States, 2Biomedical Engineering, Northwestern University, Evanston, IL, United States, 3Cardiovascular MR R&D, Siemens Medical Solutions USA, Inc, Cleveland, OH, United States, 4Cardiovascular MR R&D, Siemens Medical Solutions USA, Inc, Chicago, IL, United States, 5Siemens Healthcare, Erlangen, Germany
Synopsis
Recently, a highly accelerated compressed sensing (CS) 4D flow framework with navigator gating and retrospective ECG-gating was developed and tested in healthy volunteers and patients. This study aimed to determine the optimal protocol for high resolution (2-3 mm3) whole-heart 4D flow MRI in <8 minutes without respiratory gating, and minimization of respiratory artifacts while improving scan efficiency.
Purpose
The potential utility of cardiopulmonary evaluation of hemodynamics using 4D flow has long been known. However, whole heart 4D flow MRI applications are clinically limited by relatively low resolution (3.5-4.0 mm3 acquired spatial resolution) related to long scan times on the order of 10-18 minutes. Moreover, because the heart sits on top of the left hemisphere of the diaphragm, whole-heart imaging is particularly sensitive to respiratory motion, however even advanced navigator-gating techniques are limited to 60-80% scan efficiency. Recently, a highly accelerated compressed sensing (CS) 4D flow framework with navigator gating and retrospective ECG-gating was developed and tested in healthy volunteers and patients. Pilot studies demonstrated the feasibility of the technique for acquiring 2-minute aortic 4D flow MRI with less than 5 minutes of inline reconstruction time on the scanner.1,2 However, prior investigations into this framework have focused on aortic applications with a consistent protocol across all subjects. This study aimed to determine the optimal protocol for high resolution (2-3 mm3) whole-heart 4D flow MRI in <8 minutes with minimization of respiratory artifacts while improving scan efficiency.Methods
Study Cohort: 4D flow imaging of the heart was acquired in three healthy volunteers (all male, age=75, 37, 66 years, non-contrast), with one volunteer returning for a second set of scans (subject 2, scans 1,2 represented as 2.1 and 2.2, respectively), and one patient with a bicuspid aortic valve (post Gd-contrast, Dotarem, male, age=38 years).
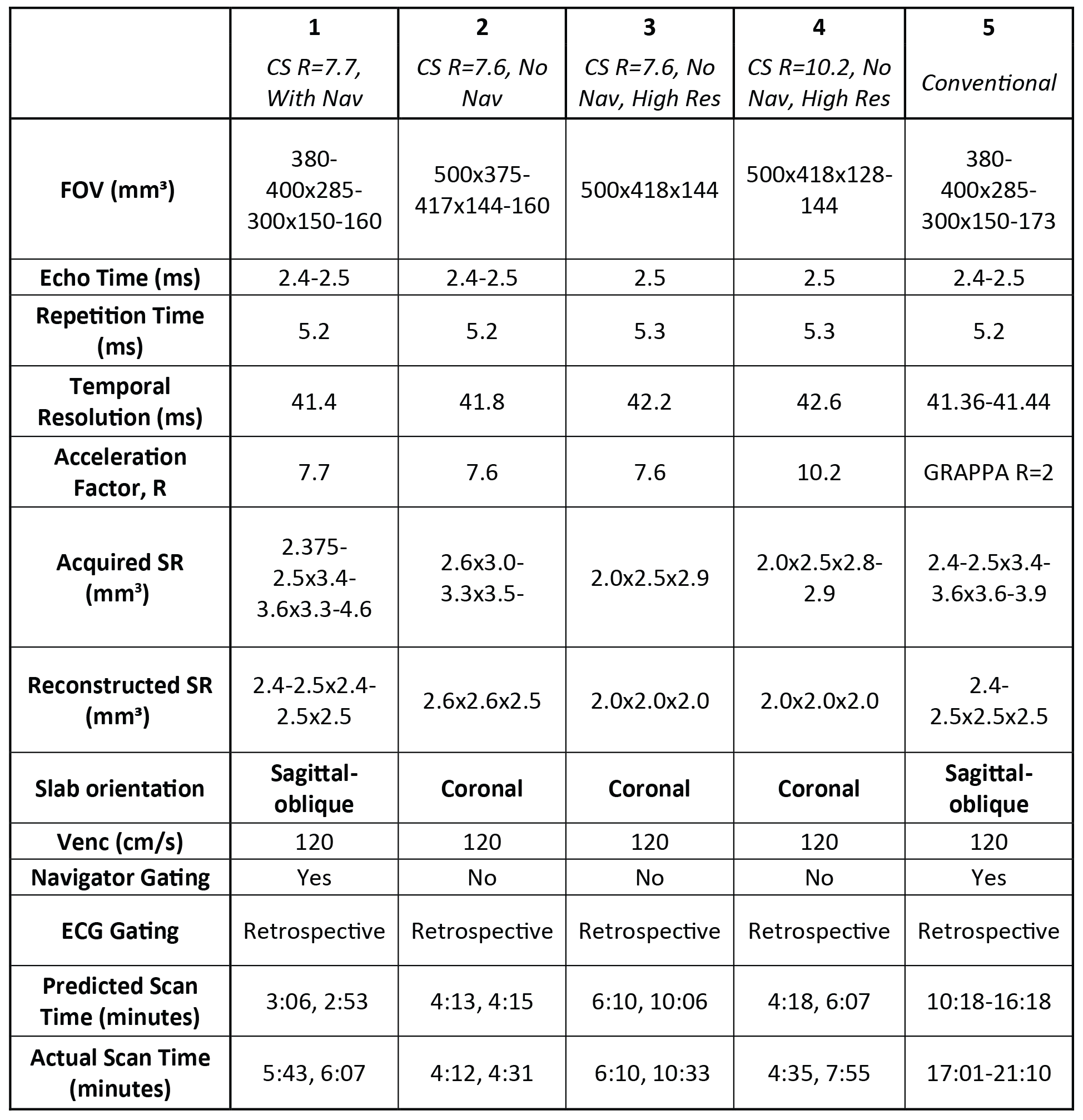
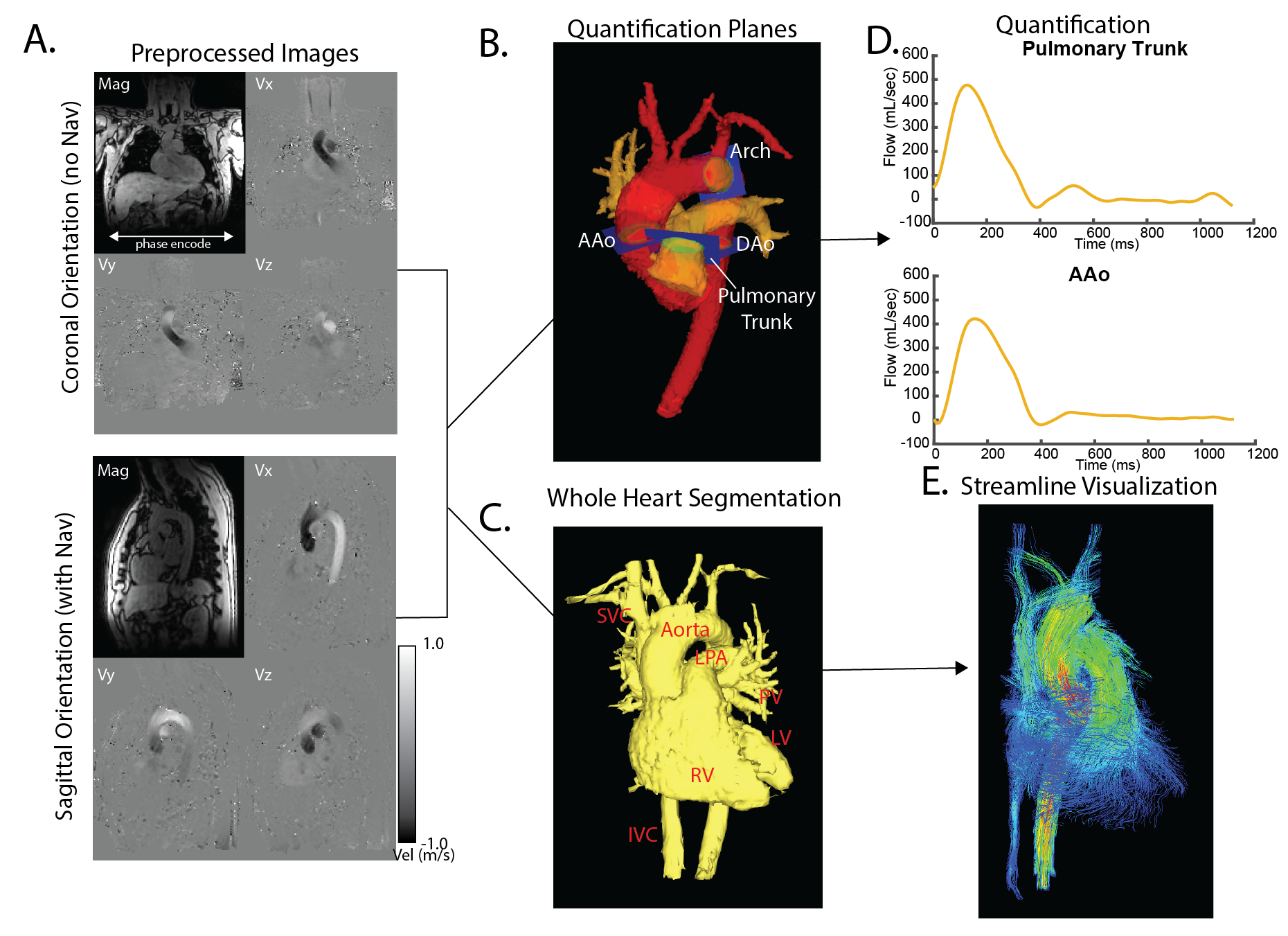
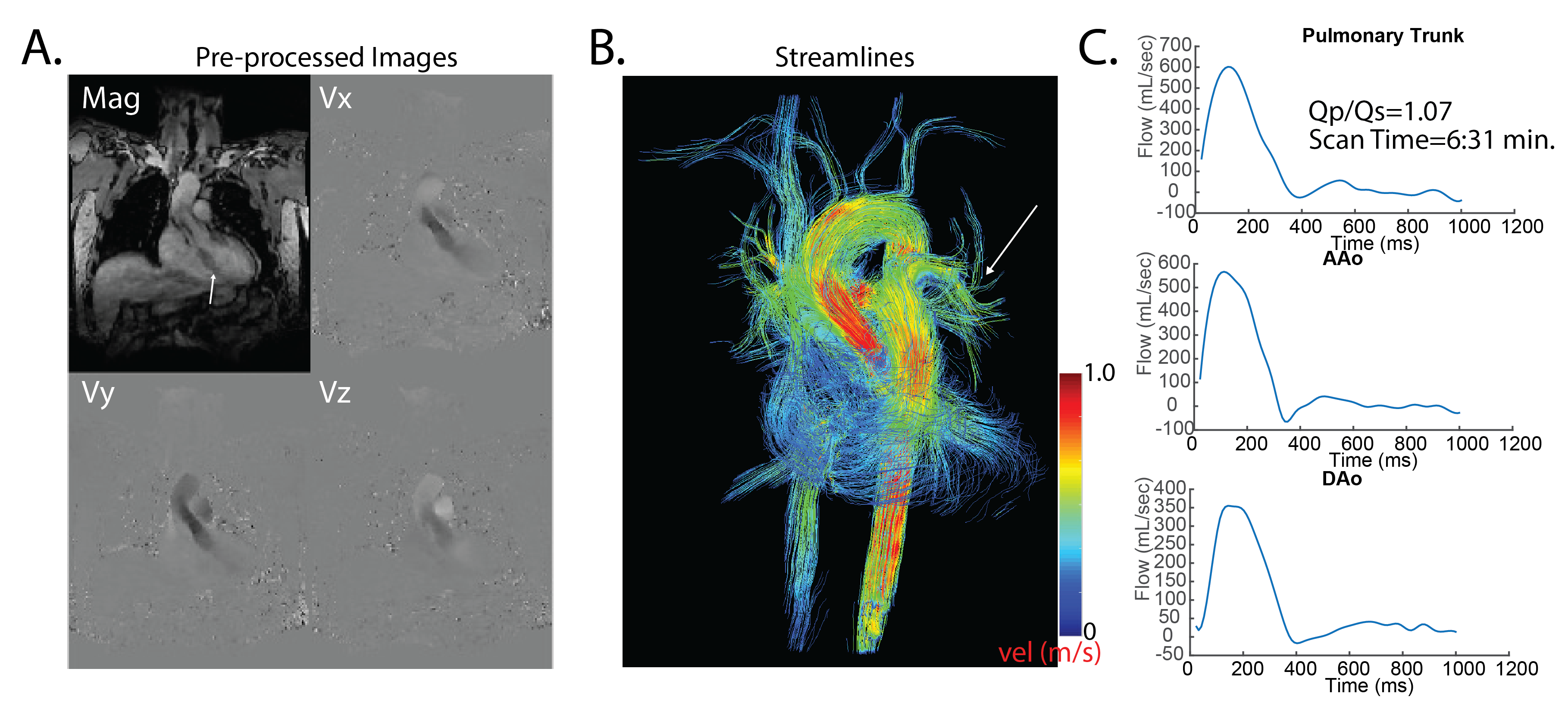
Data Acquisition: All data were acquired on a 1.5T MAGNETOM Aera (Siemens Healthcare, Erlangen, Germany) using a prototype retrospectively-gated CS 4D flow sequence. Each volunteer received two different whole-heart CS 4D flow scans with parameters delineated in Table 1. Protocols without respiration control (No Nav, 2-4) were acquired in a coronal orientation with a large field-of-view and left-right (LR) phase encode direction, perpendicular to the primary direction of diaphragmatic motion to minimize respiratory motion artifacts (Figure 1A, top). For comparison, a conventional whole-heart, sagittal-oblique 4D flow scan with R=2 GRAPPA acceleration and similar spatial and temporal resolution was acquired in all volunteers (Figure 1A, bottom). Sagittal-oblique CS 4D flow with navigator gating was also acquired in two volunteers (protocol 1).
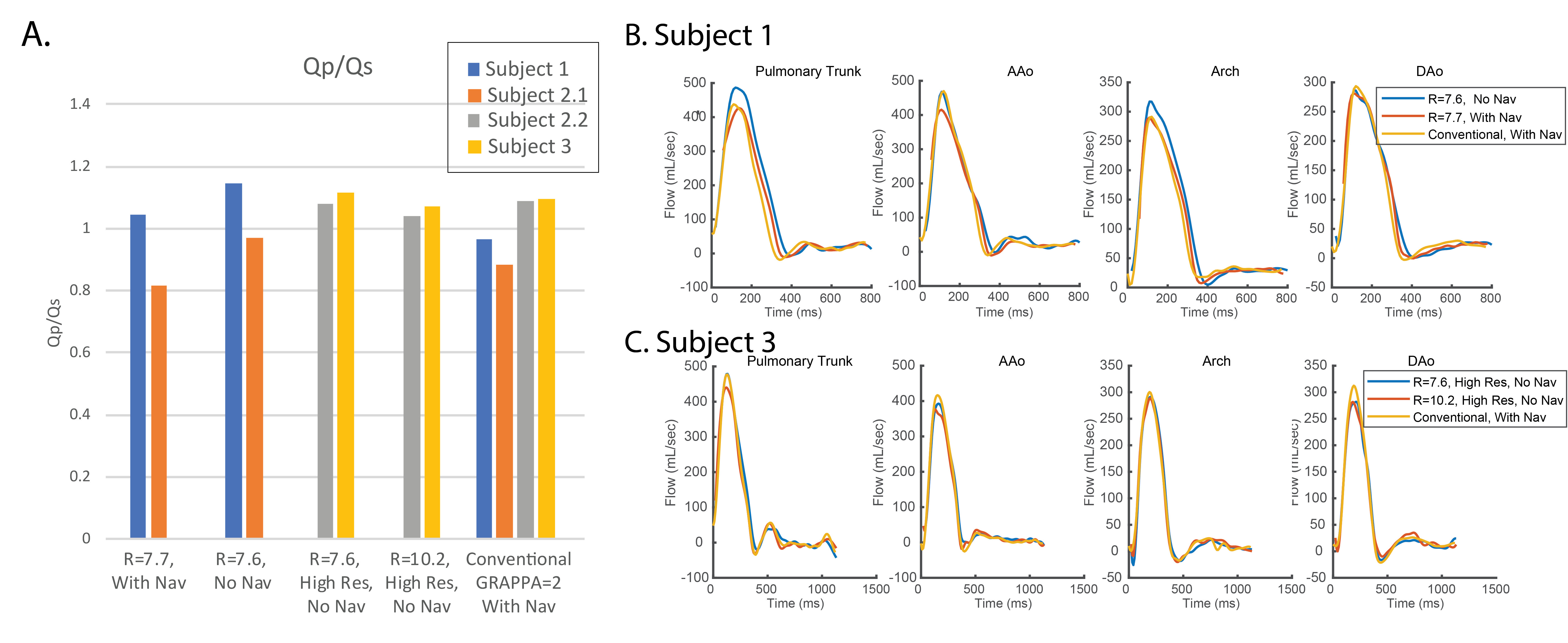
Data Analysis: Preprocessing included background phase correction, noise filtering, and anti-aliasing. 3D segmentation of the thoracic aorta and pulmonary arteries were created (Mimics, Materialise, Leuven, Belgium) based on a calculated 3D phase contrast MR-angiogram. For flow quantification, four 2D analysis planes were placed in the ascending aorta, arch, descending aorta, and pulmonary trunk (Figure 1B). Peak systolic streamlines emitted from a segmented whole heart and great vessels (Figure 1E) were compared between acquisition protocols for each volunteer. Qp/Qs (pulmonary net flow/systemic net flow) was calculated based on net flow over the proximal AAo (systemic) and pulmonary trunk (pulmonary) planes.
Results
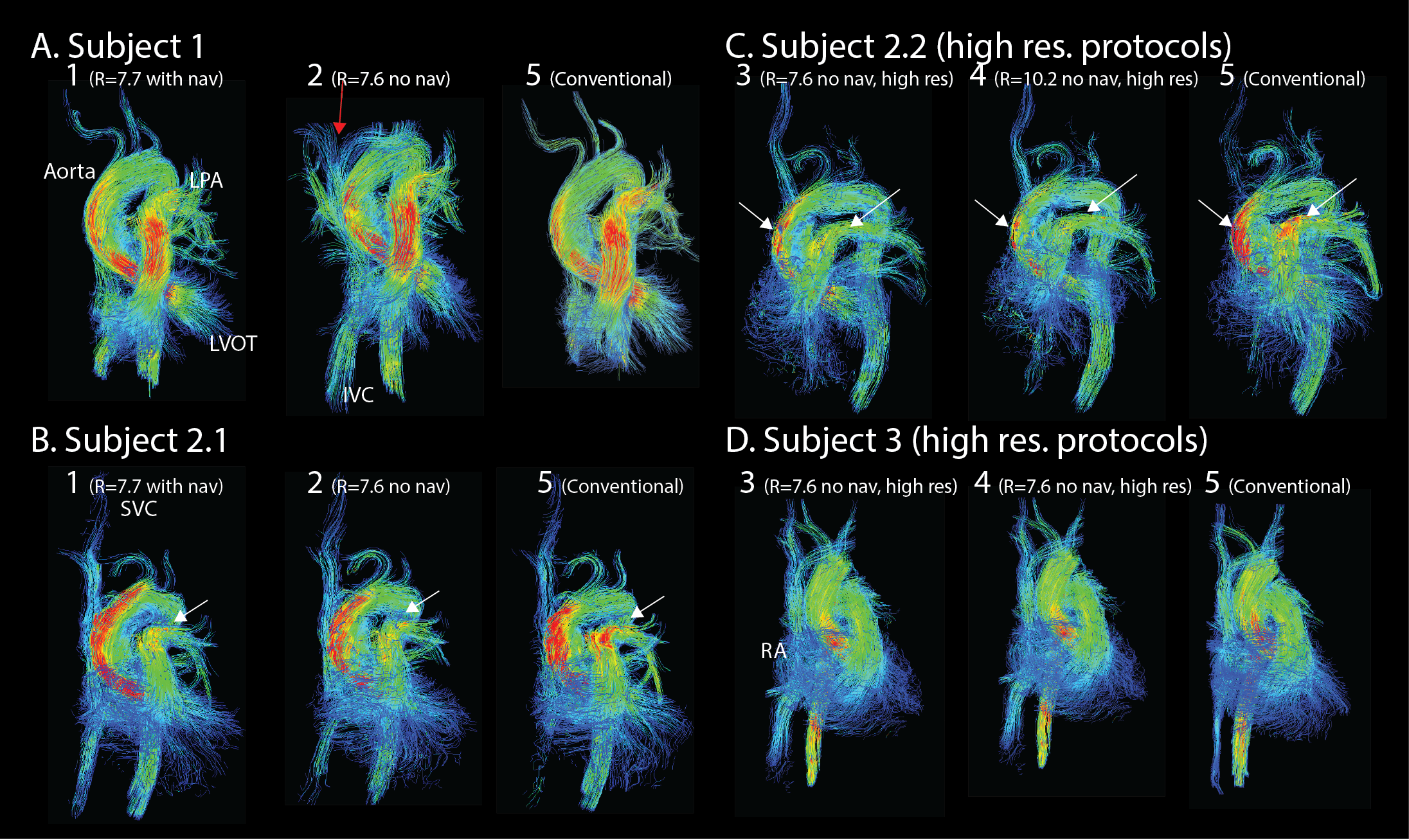
CS 4D flow reduced scan time by ~40-75% over conventional imaging protocols with about 15-20 minutes of CS online reconstruction times. While predicted scan times were shorter using protocol 1 (sagittal-oblique, CS R=7.7 with navigator), actual scan times were longer than those of protocol 2 (coronal, R=7.6, no nav). Streamline visualization (Figure 2) showed good agreement between CS with and without navigator gating (subjects 1, 2.1), CS with no navigator at different acceleration factors (subjects 2.2-3), and between CS and a conventional GRAPPA whole-heart acquisition. Qp/Qs was consistent across subjects 2.2-3 (high resolution protocols), but more variable over subjects 1-2.1. Time-resolved flow curves (Figure 3) showed agreement between CS protocols and conventional WH acquisitions, with some underestimation at higher acceleration factors in the high-resolution protocol (subject 3). Patient results (Figure 4) using protocol 4 with gadolinium contrast demonstrated improved blood-myocardium contrast and streamline visualization of smaller pulmonary branches compared to non-contrast volunteers.Discussion/Conclusions:
This study demonstrates the feasibility of highly accelerated, high resolution, whole-heart 4D flow in a <8 minute efficient imaging protocol without respiration control, with reasonable inline reconstruction time. Higher acceleration factors and resolution without respiration control (protocol 4) demonstrate similar qualitative and quantitative depiction of hemodynamics with navigator-gated conventional whole-heart 4D flow. While volunteers should have pulmonary-to-systemic flow ratios of 1, 0.05-0.2 overestimation in Qp/Qs over some imaging protocols could be explained by insufficiently corrected phase offsets based on the differing location of the pulmonary arteries and AAo. As this was only a preliminary investigation and whole-heart scans are quite long, 4 different CS whole-heart protocols were applied to 4 different volunteer scans for initial refinement of an imaging protocol. Future work will include further investigations into non-respiratory gated protocols in both sagittal-oblique and coronalorientations, the effect of increasing acceleration factors, and accuracy of Qp/Qs measurements.
Acknowledgements
National Heart, Lung, and Blood Institute of the NIH under Award F30HL137279References
1. Ma L; Chow, K.; Forman, C.; Greiser, A; Schnell, S.; Barker, A.; Markl, M.; Jin, N.; . Highly acclerated 4D flow with compressed sensing for evaluation of aortic hemodynamics. Proceedings of the Annual Meeting of the Society for Magnetic Resonance Angiography 2018; Glasgow, Scotland.
2. Jin, N; Ma, L.; Chow, K.; Forman, C.; Greiser, A; Schnell, S.; Barker, A.; Markl, M. Highly-accelerated 4D flow in the aorta with compressed sensing, respiratory controlled adaptive k-space reordering and inline reconstruction. Proceedings of the Annual Meeting of the International Society for Magnetic Resonance in Imaging 2018; Paris, France.
Figures