1987
Potential impact of pulmonary area on retrograde flow and pressure difference in patients with repaired tetralogy of Fallot1Department of Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Hsinchu, Taiwan, 2Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3Department of Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 4Department of Pediatrics, National Yang-Ming University, Taipei, Taiwan
Synopsis
The residual pulmonary regurgitation can lead to heart failure in patients with repaired tetralogy of Fallot (rTOF). We aimed to explore the possible impact of pulmonary area on pulmonary retrograde flow and pressure. Patients with rTOF presented higher retrograde flow than normal controls. The area ratio correlated with with retrograde flow in rTOF patients. Negative correlations between area ratio and pressure difference was also presented in patients. In conclusion, pulmonary area was correlated with retrograde flow and pressure difference in rTOF patients. The information of appropriate pulmonary area ratio might be helpful for treating the pulmonary stenosis in patients with rTOF.
Introduction
The residual pulmonary regurgitation can lead to right ventricular (RV) volume overload, hypertrophy, fibrosis, and heart failure in patients with repaired tetralogy of Fallot (rTOF).1,2 The pulmonary regurgitation is an important cause of late complication in rTOF patients.3 The pressure gradient can be used to evaluate the severity of aortic valve stenosis and aortic coarctation.4 The correlation between pressure and vascular geometry was reported.5 Appropriate pulmonary stenosis has been proven to be favorable for limiting hypertrophy and RV dilatation and maintaining myocardial contractility.6 The purpose of this study was to explore the possible impact of pulmonary cross-sectional area on pulmonary retrograde flow and pressure.Methods
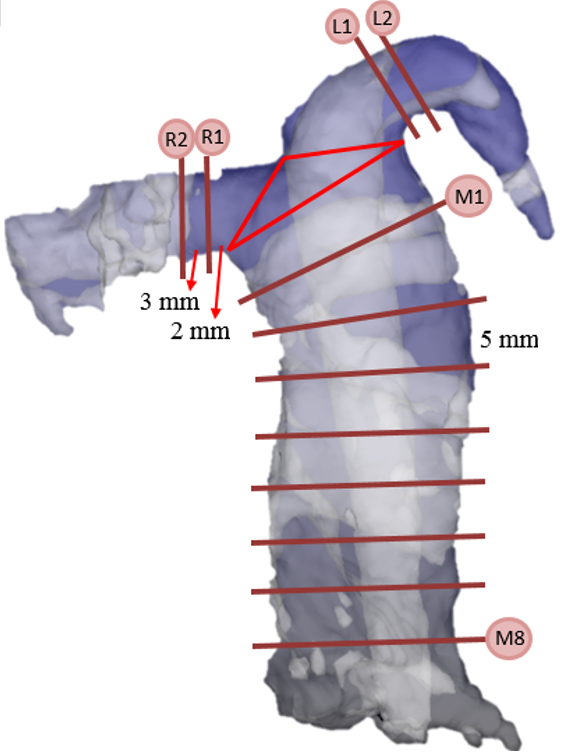
This study recruited 22 rTOF patients (22±3 y/o, male/female: 14/8) and 23 age-matched normal subjects (22±1 y/o male/female: 15/8) without known cardiovascular diseases. Images were acquired at a 3-T clinical MR scanner (Tim Trio or Skyra, Siemens, Erlangen, Germany) with prospective ECG triggering and navigator-echo to synchronize with cardiac and respiratory motion. 4D flow was acquired by TR/TE=10.8/2.9 ms, voxel size=3.2x1.4x3.5 mm3, flip angle=7°, Venc=150 cm/s, and temporal resolution=41.6 ms. We determined 12 planes in main, right and left pulmonary arteries (MPA, RPA, LPA) (Figure 1). The pulmonary retrograde flow fraction was calculated as the percentage of retrograde flow volume/antegrade flow volume.7 The pressure difference,Δp, between each plane and M8 was calculated using the simplified Bernoulli equation 8 : Δp = 4Vmax2 , where Vmax represents the maximum velocity during cardiac cycle. An area ratio was defined as the cross-sectional area of each plane normalized by the area of M8. Two-tailed Student t test and Pearson correlation were performed when appropriate. P<0.05 was considered as statistical significance.Results
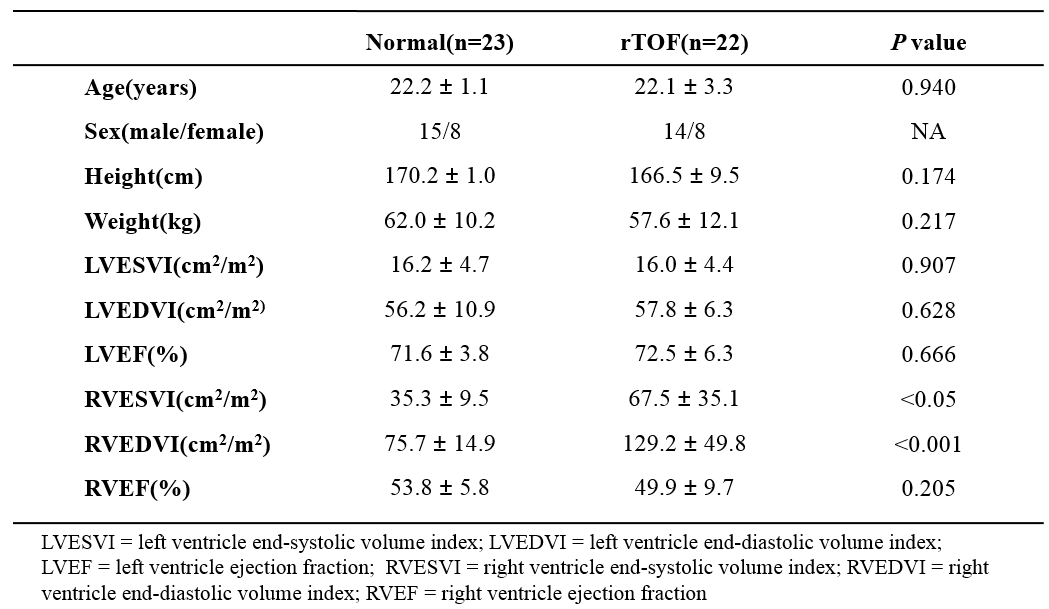
Table 1 summarizes
the demographics of the study population. Patients presented higher RV
end-systolic volume index (P<0.05) and end-diastolic volume index
(P<0.01), representing the presence of dilated RV in rTOF patients. Nevertheless,
the rTOF group had preserved RV ejection fraction (RVEF) and LVEF.
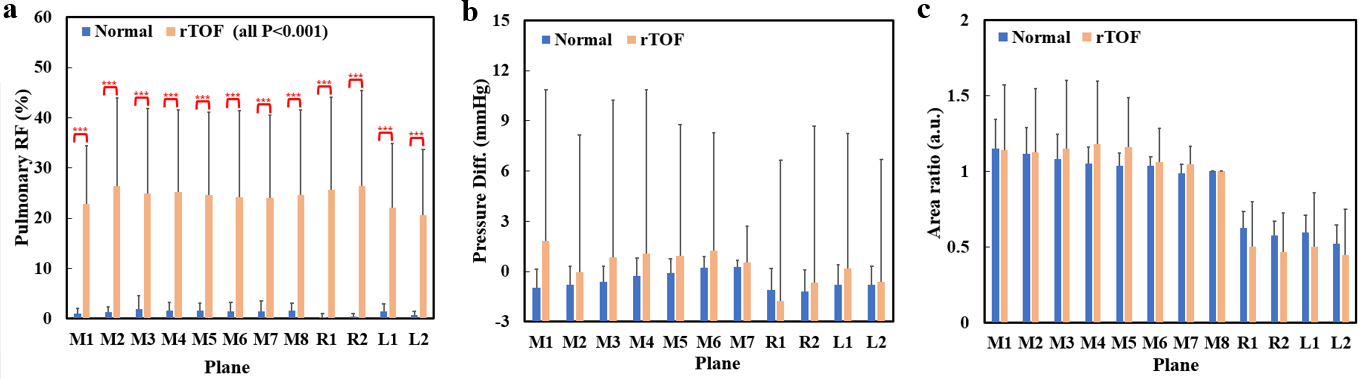
As show in Figure 2, rTOF patients have
significantly higher retrograde flow than normal controls (P<0.001). There
is no significant difference of pressure differences and area ratio between
rTOF and normal groups.
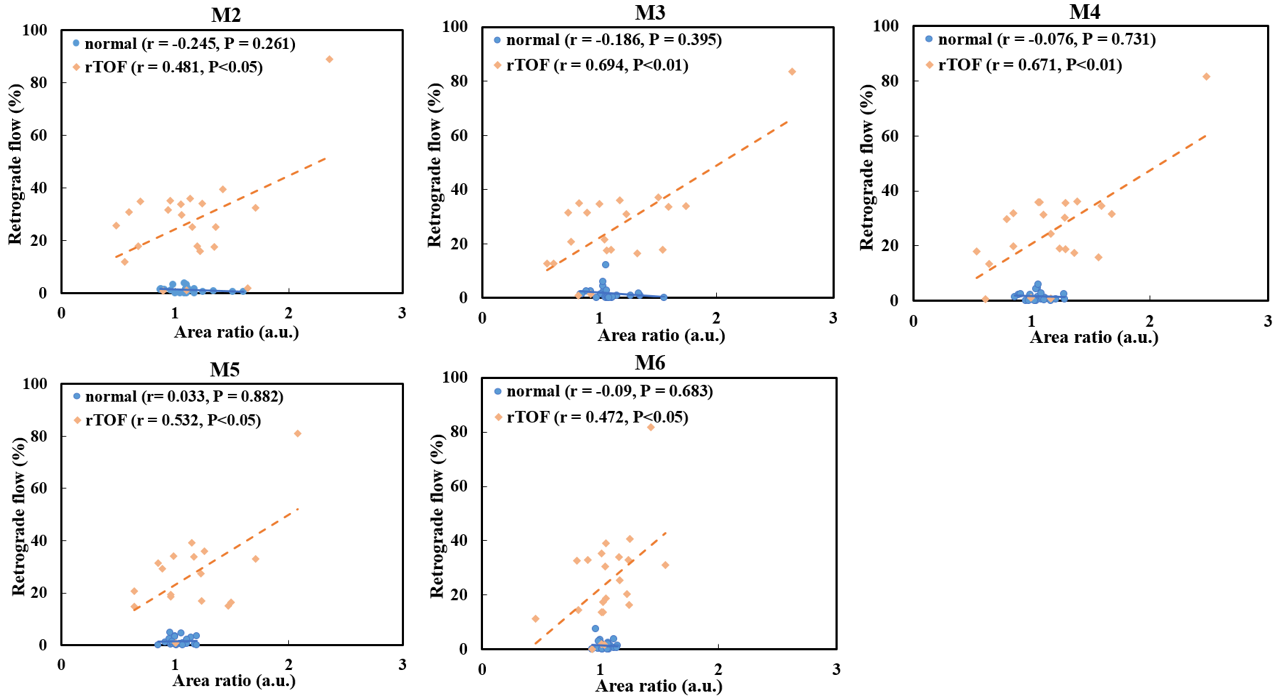
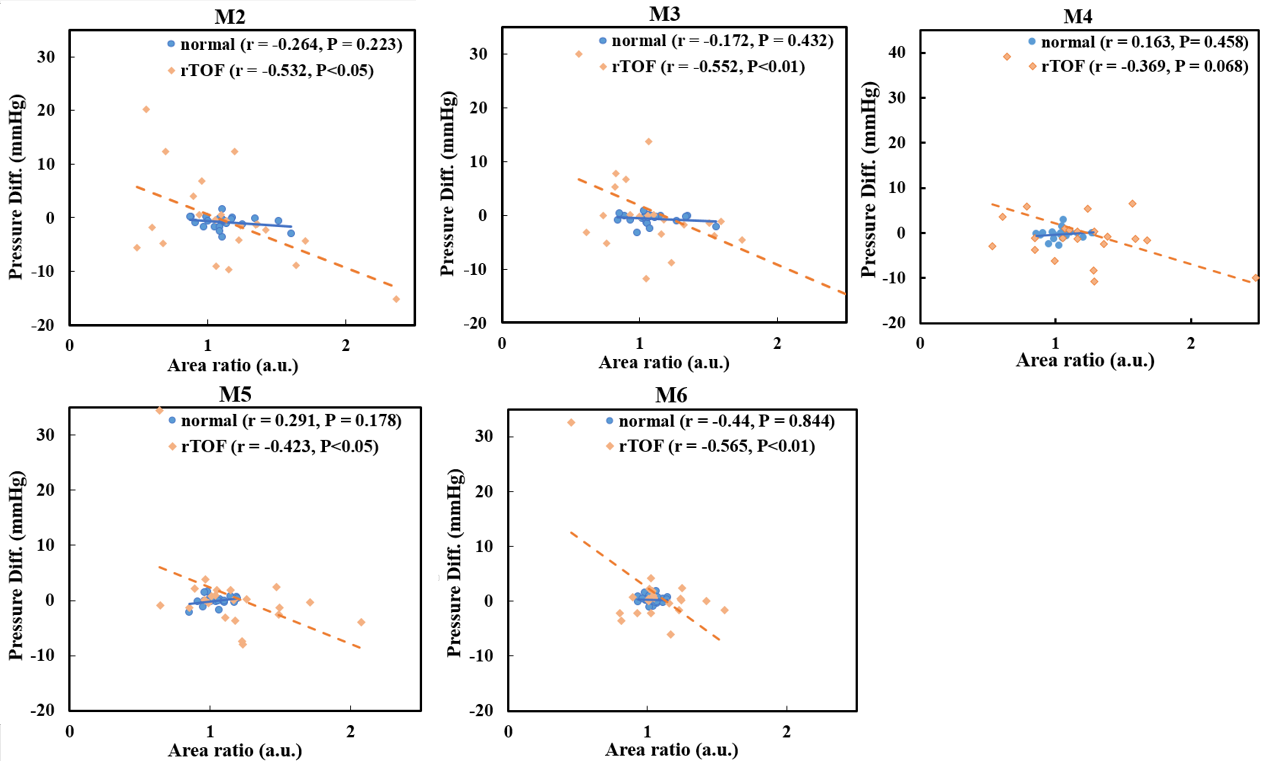
Figure 3 shows significantly positive
correlations between the retrograde flow and area ratio in the M2-M6 of rTOF
patients (r = 0.47-0.69, P<0.05). The negative correlation between pressure
difference and area ratio was also presented in M2-M6, except M4, (r = -0.48–-0.57, P<0.05), as shown in Figure 4.
Discussion and Conclusion
In this study, we calculated pulmonary
retrograde flow, pressure difference, and pulmonary cross-sectional area in
rTOF patients and found correlations in-between.
The mitral regurgitation was positively correlated with maximal jet
area.9 Patients with rTOF frequently encounter pulmonary
regurgitation and/or residual or recurrent pulmonary artery stenosis.10
In this study, the area ratio in rTOF group was comparable with normal group
but moderate positive correlations were shown between area ratio and retrograde
flow solely in rTOF group. This finding suggested that maintaining smaller area
ratio, i.e. appropriate pulmonary stenosis, could overcome pulmonary
regurgitation and was favorable for rTOF patients. Archie, Joseph P., et
al. demonstrated that pressure loss increased with stenosis severity.11
In our study, we observed a significantly negative correlation between
pulmonary pressure difference and cross-sectional area. In conclusion,
pulmonary cross-sectional area was correlated with retrograde flow and pressure
difference in rTOF patients. The information of appropriate pulmonary area
ratio might be helpful for treating the pulmonary stenosis in patients with
rTOF.
Acknowledgements
No acknowledgement found.References
1. Chaturvedi, Rajiv R., et al. Pulmonary regurgitation in congenital heart disease. Heart. 2007; 93.7: 880-889.
2. Köhler, Doreen, et al. Right ventricular failure and pathobiology in patients with congenital heart disease–implications for long-term follow-up. Frontiers in pediatrics. 2013; 1:37.
3. Discigil, Beren, et al. Late pulmonary valve replacement after repair of tetralogy of Fallot. The Journal of thoracic and cardiovascular surgery. 2001; 121.2: 344-351.
4. Bock, Jelena, et al. In vivo noninvasive 4D pressure difference mapping in the human aorta: phantom comparison and application in healthy volunteers and patients. Magnetic resonance in medicine. 2011; 66.4:1079-1088.
5. Novakova, Ludmila, et al. Vascular stenosis asymmetry influences considerably pressure gradient and flow volume. Physiological research. 2016; 65.1:63.
6. Karl, Tom R., et al. Tetralogy of Fallot: Current surgical perspective. Annals of pediatric cardiology. 2008; 1.2:93.
7. Wehrum, Thomas, et al. Aortic atherosclerosis determines increased retrograde blood flow as a potential mechanism of retrograde embolic stroke. Cerebrovascular Diseases. 2017; 43.3-4:132-138.
8. DeGroff, C. G., et al. Accuracy of the Bernoulli equation for estimation of pressure gradient across stenotic Blalock–Taussig shunts: an in vitro and numerical study. Pediatric cardiology. 2000; 21.5:439-447.
9. Spain, Michael G., et al. Quantitative assessment of mitral regurgitation by Doppler color flow imaging: angiographic and hemodynamic correlations. Journal of the American College of Cardiology. 1989; 13.3:585-590.
10. François, Christopher J., et al. 4D cardiovascular magnetic resonance velocity mapping of alterations of right heart flow patterns and main pulmonary artery hemodynamics in tetralogy of Fallot. Journal of Cardiovascular Magnetic Resonance. 2012; 14.1:16.
11. Archie, Joseph P., et al. Analysis and comparison of pressure gradients and ratios for predicting iliac stenosis. Annals of vascular surgery. 1994; 8.3: 271-280.
Figures