1986
Interaction between pulmonary flow and myocardial motion in patients with repaired tetralogy of Fallot1Department of Biomedical Engineering and Environmental Sciences, National Tsing Hua University, Hsinchu, Taiwan, 2Department of Radiology, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3Department of Pediatrics, Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 4Department of Pediatrics, National Yang-Ming University, Taipei, Taiwan
Synopsis
We aimed to investigate the interaction between pulmonary flow and myocardial motion in patients with repaired tetralogy of Fallot (rTOF). The 4D flow MRI and tissue phase mapping were employed to quantify the pulmonary flow and myocardial motion velocity, respectively. The pulmonary retrograde flow was correlated with left ventricular (LV) peak diastolic longitudinal velocity and time-to-peak (Vz and TTPz) in rTOF patients. Pulmonary pulsatility index was correlated with diastolic RV TTPr and LV TTPz. In conclusion, the correlation between abnormal pulmonary artery flow and altered myocardial motion may provide helpful information in evaluating the cardiac function in rTOF patients.
Introduction
For patients with repaired tetralogy of Fallot (rTOF), chronic pulmonary regurgitation (PR) contributes to irreversible right ventricle (RV) failure.1, 2 4D flow MRI was used to quantify flow-related parameters in a variety of cardiovascular diseases.3 Tissue phase mapping (TPM) was used to measure myocardial motion velocity in patients with left ventricular (LV) hypertrophy.4 The impaired LV function was proven to be related to PR and RV dilatation in rTOF patient.5-7 The myocardial deformation was reported to be superior to conventional ventricular function for predicting the outcome in rTOF patients.8 On the other hand, the increased pulmonary pulsatility index (PI) was employed to evaluate global RV function and predict RV failure in continuous-flow left ventricular assist device implantation patients.9 Currently, the regional myocardial motion and its correlation with pulmonary flow in rTOF has not been discussed. The purpose of this study was to investigate the abnormal pulmonary artery flow and adverse interaction with regional myocardial motion in rTOF patients with preserved RV ejection fraction (RVEF) and LVEF.Methods
21 rTOF patients (age=23±3 y, male/female=14/7) and 18 age-matched normal controls without known cardiovascular diseases (age=22±1 y, male/female=12/6) were recruited. Images were acquired at a 3-T clinical MR scanner (Tim Trio or Skyra, Siemens, Erlangen, Germany) with prospective ECG triggering and navigator-echo to synchronize with cardiac and respiratory motion. 4D flow was acquired by TR/TE=10.8/2.9 ms, voxel size=3.2x1.4x3.5 mm3, flip angle=7°, Venc=150 cm/s, and temporal resolution=41.6 ms. For myocardial motion velocity, all subjects were imaged in base, mid, and apex with parameters of TR/TE=6.5/4.2 ms, voxel size=1.17x1.17x6 mm3, flip angle=7°, acceleration factor=5, Venc=15 and 25 cm/s for in-plane and through-plane motions, respectively, and temporal resolution=26 ms. We determined 12 planes in main, right and left pulmonary arteries (MPA, RPA, LPA) (Figure 1). The pulmonary pulsatility index (PI), representing the vascular resistance, is defined as: PI=(peak systolic velocity – end-diastolic velocity)/time-averaged maximum velocity.10 The pulmonary retrograde flow (RF) is defined as: RF = retrograde flow volume/antegrade flow volume.11 Biventricular peak systolic and diastolic myocardial velocity in radial (Vr) and longitudinal (Vz) directions and the corresponding time-to-peak (TTPr, TTPz) were also computed. Two-tailed Student t test and Pearson correlation were performed when appropriate. P < 0.05 was considered as statistical significance.Results
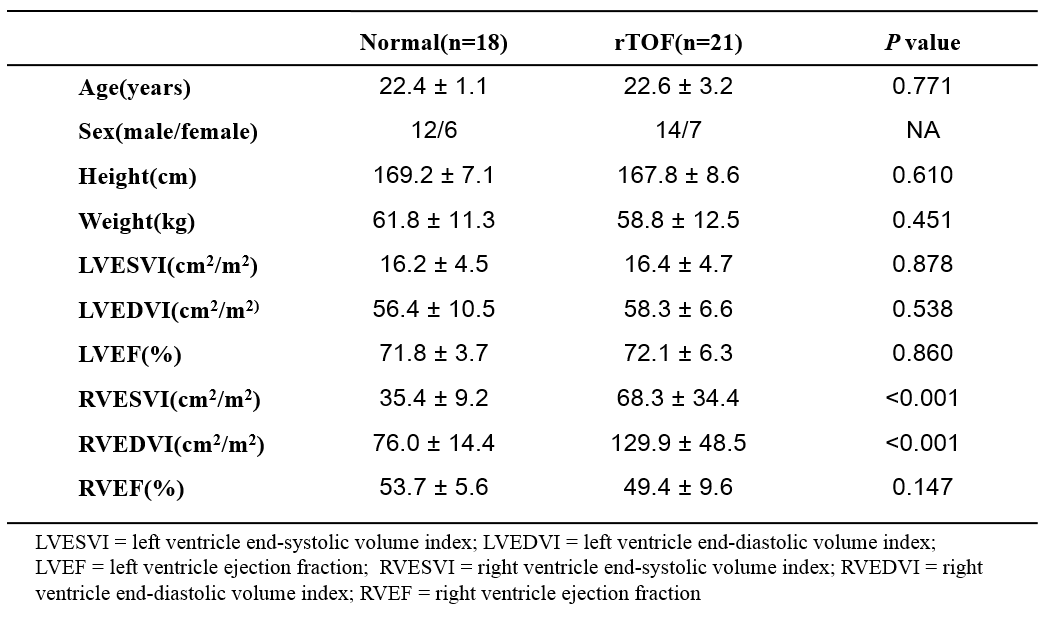
In Table 1, rTOF group presented higher RV end-systolic and end-diastolic volume index than normal group (both P < 0.001), indicating the dilated RV in rTOF patients. Nevertheless, rTOF group demonstrated preserved RVEF and LVEF. Figure 2 illustrates higher pulmonary RF (P<0.001) and PI (P<0.01~0.001) in rTOF patients than normal controls. The pulmonary RF in rTOF patients was correlated with LV diastolic Vz in M1~M7 in MPA (r=0.44~0.50, all P<0.05) and in RPA (r=0.58~0.59, both P<0.05). Patients with rTOF also presented strong correlation between the pulmonary RF and LV diastolic TTPz in all selected planes of the MPA, RPA, and LPA (r=0.65~0.80, all P<0.01). The pulmonary PI of rTOF patients demonstrated moderate to strong correlations with RV diastolic TTPr almost in all selected planes (r=0.44~0.70, all P<0.05). The correlation between pulmonary PI and LV diastolic TTPz were also significant in all selected planes (r=0.42~0.79, all P<0.05). There is no significant correlation of abovementioned indices shown in normal controls. Figure 3 demonstrates the high correlations of abovementioned indices in the M7 of MPA.Discussion and Conclusion
In this study, we observed the correlations of pulmonary artery flow and myocardial motion in rTOF patients. Long QRS duration, abnormal RV dilatation, and severe PR are associated with RV dysfunction in rTOF patients.12 The rTOF patients in this study were with dilated RV and substantial pulmonary RF but preserved LVEF and RVEF, reflecting the relatively early disease stage. The positive correlation between pulmonary RF and LV diastolic Vz and TTPz depicted that PR might also affect the LV myocardial motion and maintaining a lower LV diastolic Vz and shorter LV diastolic TTPz than normal controls might be favorable for rTOF patients. The correlation between pulmonary PI and RV diastolic TTPr as well as LV diastolic TTPz in the rTOF group indicated the possible interaction between pulmonary flow and bi-ventricular myocardial motion while patients were in an early disease stage. Part of rTOF patients with higher PI were also prolonged LV diastolic TTPz rather in TTPr, reflecting that altered pulmonary flow might first impact on the longitudinal fiber which was consistent with the previous study.13 In conclusion, the correlation between abnormal pulmonary artery flow and altered myocardial motion may provide helpful information in evaluating the cardiac function in patients with rTOF in an early disease stage.Acknowledgements
No acknowledgement found.References
1. McElhinney, Doff B., et al. Pulmonary valve replacement in tetralogy of Fallot: impact on survival and ventricular tachycardia. Circulation. 2009; 119(3):445-51.
2. Hickey, Edward J., et al. Late risk of outcomes for adults with repaired tetralogy of Fallot from an inception cohort spanning four decades. Eur J Cardiothorac Surg. 2009; 35(1):156-64.
3. Stankovic, Zoran, et al. 4D flow imaging with MRI. Cardiovasc Diagn Ther. 2014; 4(2):173-92.
4. Jung, Bernd, et al. Detailed analysis of myocardial motion in volunteers and patients using high‐temporal‐resolution MR tissue phase mapping. J Magn Reson Imaging. 2006; 24(5):1033-9.
5. Davlouros, Periklis A., et al. Right ventricular function in adults with repaired tetralogy of Fallot assessed with cardiovascular magnetic resonance imaging: detrimental role of right ventricular outflow aneurysms or akinesia and adverse right-to-left ventricular interaction. J Am Coll Cardiol. 2002; 40(11):2044-52.
6. Nakamura, Akihiro, et al. Right ventricular remodeling due to pulmonary regurgitation is associated with reduced left ventricular free wall strain in surgically repaired tetralogy of fallot. Circ J. 2014; 78(8):1960-6.
7. Diller, Gerhard-Paul, et al. Left ventricular longitudinal function predicts life-threatening ventricular arrhythmia and death in adults with repaired tetralogy of fallot. Circulation. 2012; 125(20):2440-6.
8. Orwat, Stefan, et al. Myocardial deformation parameters predict outcome in patients with repaired tetralogy of Fallot. Heart. 2016; 102(3):209-15.
9. Morine, Kevin J., et al. Pulmonary Artery Pulsatility Index Is Associated With Right Ventricular Failure After Left Ventricular Assist Device Surgery. Journal of Cardiac Failure. 2016; 22(2):110-6.
10. Gudmundsson, Saemundur, et al. Placental pulsatility index: a new, more sensitive parameter for predicting adverse outcome in pregnancies suspected of fetal growth restriction. Acta Obstet Gynecol Scand. 2017; 96(2):216-222.
11. Wehrum, Thomas, et al. Aortic Atherosclerosis Determines Increased Retrograde Blood Flow as a Potential Mechanism of Retrograde Embolic Stroke. Cerebrovasc Dis. 2017; 43(3-4):132-138.
12. van den Berg, Jochem, et al. Clinical condition at mid-to-late follow-up after transatrial-transpulmonary repair of tetralogy of Fallot. J Thorac Cardiovasc Surg. 2007; 133(2):470-7.
13. Davlouros, Periklis A., et al. Right ventricular function in adults with repaired tetralogy of Fallot assessed with cardiovascular magnetic resonance imaging: detrimental role of right ventricular outflow aneurysms or akinesia and adverse right-to-left ventricular interaction. J Am Coll Cardiol. 2002; 40(11):2044-52.
Figures