1985
Non-Invasive Evaluation of Inhaled Nitric Oxide on Pulmonary Blood Flow Dynamics using 4D Flow MRI in Pediatric Pulmonary Arterial Hypertension Patients1Radiology, Children's Hospital Colorado, Aurora, CO, United States, 2Cardiology, Children's Hospital Colorado, Aurora, CO, United States, 3Pediatrics, Children's Hospital Colorado, Aurora, CO, United States, 4Bioengineering, University of Colorado Denver, Aurora, CO, United States
Synopsis
Pediatric pulmonary arterial hypertension (PAH) is a significant cause of morbidity and mortality. Acute vasodilatory reactivity (AVR) using right heart catheterization is a necessary component of a diagnostic PAH evaluation. The aim of this study was to non-invasively evaluate AVR hemodynamic changes in pediatric patients with PAH using 4D flow MRI. We have shown that post-iNO treatment in pediatric PAH patients, peak velocity and peak wall shear stress were increased. Future studies in larger cohorts of PAH pediatric patients are needed to comprehensively evaluate the effectiveness of non-invasive AVR in comparison to gold standard right heart catheterization.
Introduction
Pediatric pulmonary arterial hypertension (PAH) is a significant cause of morbidity and mortality and is characterized by remodeling of the pulmonary vasculature, ultimately leading to right heart failure. Acute vasodilatory reactivity (AVR) using right heart catheterization is a necessary component of a diagnostic PAH evaluation, which assesses disease severity, determines the route of therapy, and is prognostic of survival (1,2). Given that 4D flow MRI can be used to non-invasively evaluate complex hemodynamic changes in the pulmonary arteries (3), and that parameters such as wall shear stress (WSS) have been shown to be critical in vascular remodeling processes, the aim of this study was to non-invasively evaluate AVR hemodynamic changes in pediatric patients with PAH using 4D flow MRI.Methods
24 4D flow MRI exams were performed in pediatric PAH patients (N = 12) before and after inhalation of FiO2 1.0 and iNO 40ppm for 10 minutes on a 3T scanner (Ingenia, Philips Medical Systems, Best, The Netherlands) using ECG gating and respiratory navigator in a sagittal oblique 3D volume covering the mid-thorax. Typical pulse sequence parameters included: TE/TR = 2.5-2.8/4.0-4.6 ms, flip angle = 100, temporal resolution = 38-48 ms, VENC = 150 cm/s, spatial resolution = 2.6 x 2.6 x 2.2-2.8 mm3. 4D flow MRI post-processing was performed using a CVI42 platform (Version 5.9.1, Circle Cardiovascular Imaging, Calgary, AB, Canada). Pre-processing included correction for eddy current, noise and velocity aliasing. Planes were placed perpendicular to the direction of flow in the main pulmonary artery (MPA), right pulmonary artery (RPA) and left pulmonary artery (LPA). Blood flow analyses for each plane included: stroke volume (SV), peak flow (Qmax), peak velocity (Vmax), peak WSS (i.e. WSSmax) and average wall shear stress (WSSavg). Pulmonary vascular resistance index (PVRi) and mean pulmonary artery pressures (mPAP) were measured during catheterization. Blood flow parameters, mPAP and PVRi pre and post NO inhalation were compared using paired samples t-test.Results
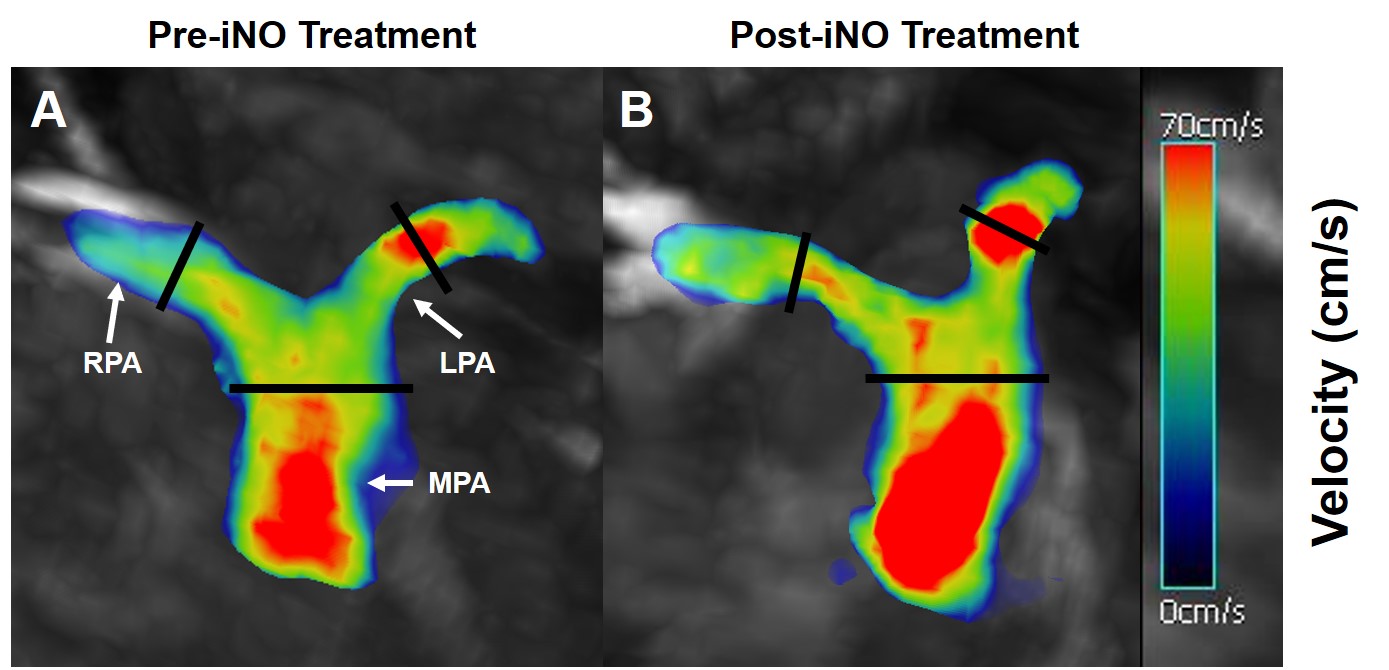
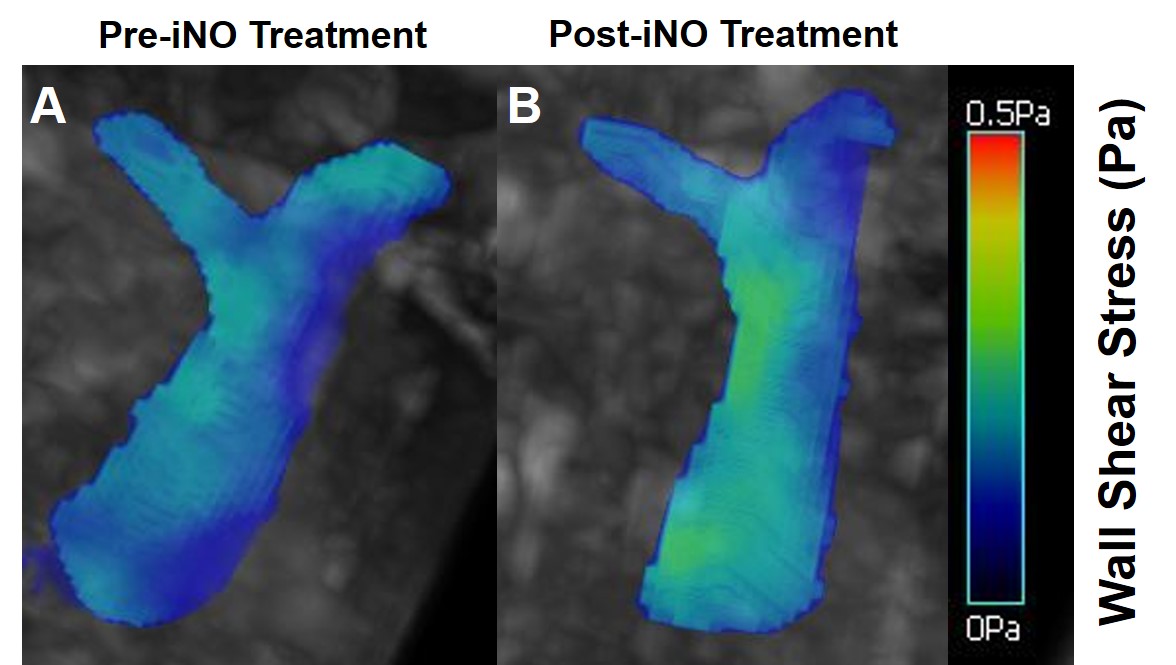
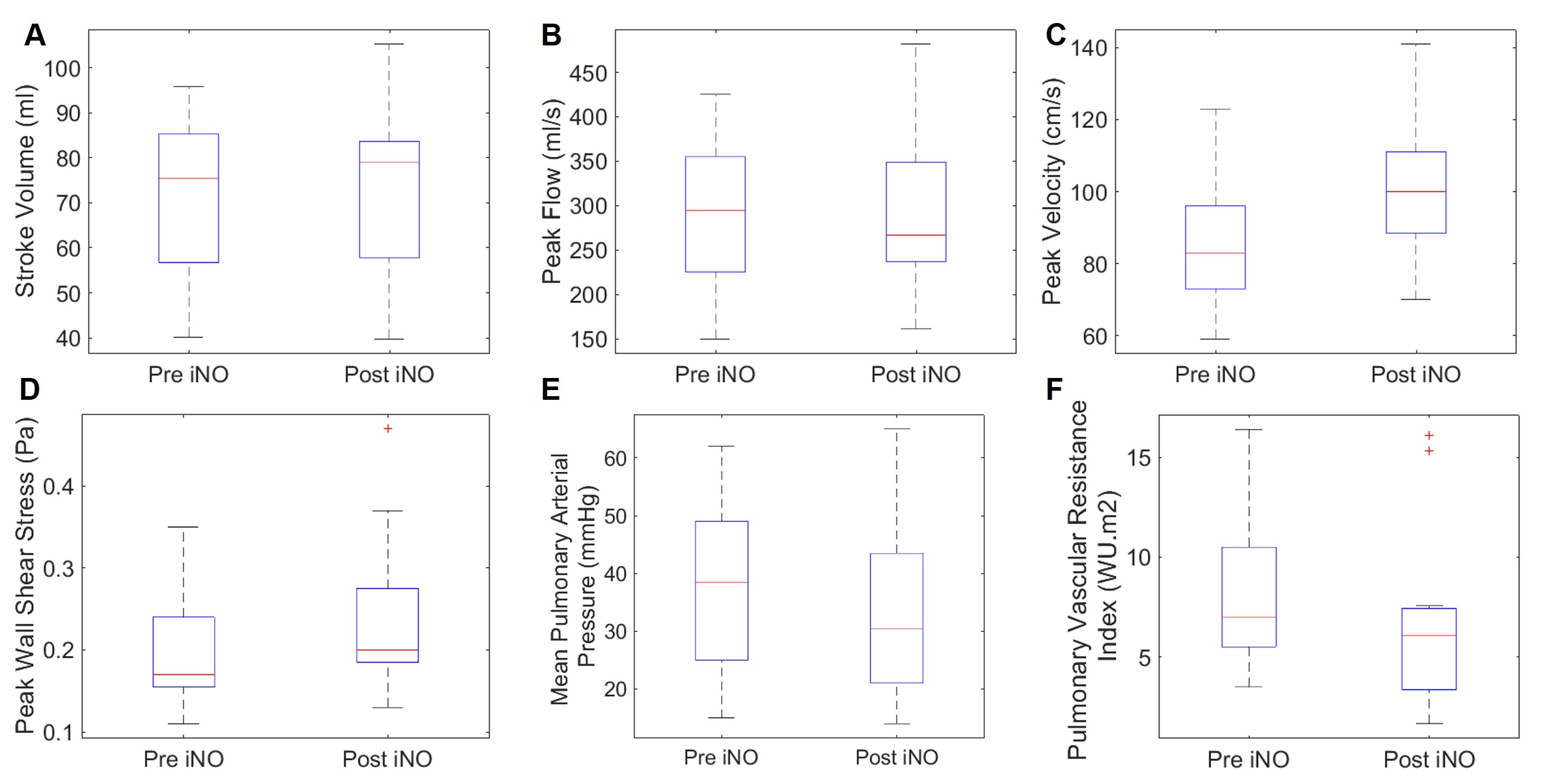
Table 1 summarizes patient demographics and mPAP and PVRi measurements obtained during catheterization. mPAP was reduced post-iNO (p<0.05 vs. pre-iNO) and there was a trend towards reduced PVRi post-iNO (p=0.08). Table 2 summarizes the various blood flow parameters obtained using 4D flow (mean ± standard deviation). Post-iNO, Vmax and WSSmax were significantly increased in MPA (p <0.05 vs. pre-iNO). There were no statistical differences in the other blood flow parameters due to NO inhalation. Figure 1 shows an example velocity map measured pre- and post-iNO where the peak velocity was increased post iNO. Figure 2 shows an example wall shear stress map measured pre and post-iNO. Figure 3 shows box plots summarizing the blood flow hemodynamics measured in MPA. Comparison of blood flow parameters derived from 4D flow with mPAP and PVRi revealed a positive correlation between mPAP and Qmax both pre-iNO (R=0.6, p=0.044) and post-iNO treatment (R=0.8, p=0.004). There was a trend towards a positive correlation between the change in PVRi and WSSavg (R=0.5, p=0.06). There was no change in PA diameter post-iNO.Conclusions
Using 4D flow MRI, it has been previously shown that peak systolic velocity and wall shear stress are lowered in PAH (3). Here, we investigate an intervention which assess vascular reactivity (AVR). In pediatric PAH patients iNO appears to result in significant changes in pulmonary flow parameters which can be measured using the 4D flow MRI technique. Specifically, we have shown that post-iNO treatment in pediatric PAH patients, Vmax and WSSmax were increased, the latter coming back towards the value seen in previously described normotensive controls. Ongoing recruitment of PAH pediatric patients is occurring and pilot data from this prospective vascular reactivity 4D flow study indicate the value of non-invasive AVR by MRI. Ongoing comparison to the gold standard, invasive right heart catheterization, is occurring and we continue to investigate the effect of vasodilators in modulating remodeling processes.Acknowledgements
No acknowledgement found.References
1. Humbert M, Morrell NW, Archer SL, Stenmark KR, MacLean MR, Lang IM, Christman BW, Weir EK, Eickelberg O, Voelkel NF, Rabinovitch M. Cellular and molecular pathobiology of pulmonary arterial hypertension. J Am Coll Cardiol. 2004 Jun 16;43(12 Suppl S):13S-24S.
2. Khambadkone S, Li J, de Leval MR, Cullen S, Deanfield JE, Redington AN. Basal pulmonary vascular resistance and nitric oxide responsiveness late after Fontan-type operation. Circulation. 2003 Jul 1;107(25):3204-8. Epub 2003 Jun 2
3. Alex J Barker, Alejandro Roldán-Alzate, Pegah Entezari, Sanjiv J. Shah, Naomi C Chesler, Oliver Wieben, Michael Markl, and Christopher J François. 4D Flow Assessment of Pulmonary Artery Flow and Wall Shear Stress in Adult Pulmonary Arterial Hypertension: Results from Two Institutions. Magn Reson Med. 2015 May; 73(5): 1904–1913.
Figures