1983
Displaced aortic flow and increased circumferential wall shear stress associate with ascending aortic dilatation in tricuspid aortic valve patients – a prospective clinical studyS. Petteri Kauhanen1, Marja Hedman1, Pekka Jaakkola2, Ritva Vanninen1, Petri Saari1, and Timo Liimatainen3
1Clinical Radiology, Kuopio University Hospital, Kuopio, Finland, 2Heart and Thoracic surgery, Kuopio University Hospital, Kuopio, Finland, 3Research Unit of Medical Imaging, Oulu University, Oulu, Finland
Synopsis
Four-dimensional (4D) flow was measured in 20 patients with dilated ascending aorta (AA) and in 20 controls. Aortic flow was displaced from the center line of the AA in patients with AA dilatation. Flow displacement was present in the proximal and tubular parts of AA. Total wall shear stress (WSS) was higher on the displaced side compared to the opposite side of the aorta. The circumferential WSS (WSSC) ratio to total WSS was higher in the inner curvature of dilated AA in the proximal part and WSSc was elevated in the whole aortic ring in the distal part of AA.
Introduction
In the dilated AA, altered blood flow velocities and displaced flow patterns have been reported (1). In patients with dilated AA with tricuspid aortic valve (TAV), total WSS values are lower as compared to those with non-dilated AA (2-4). The aim of the present study was to detect 4D flow MRI characteristics that are related to AA dilatation by comparing subjects with dilated AA to non-dilated AA in case of tricuspid aortic valve.Methods
This prospective study included consecutive patients who were scheduled for follow-up due to dilated AA (diameter ≥ 42 mm) and who had TAV (n=20). The control group included 20 healthy volunteers with TAV without AA dilatation (AA diameter < 42 mm). The baseline characteristics of the study subjects are shown in Table 1. Anatomic images and 4D flow data were acquired using Siemens MAGNETOM Aera, 1.5 T (Siemens GmbH, Erlangen, Germany) scanner. Flow was evaluated in 10 planes (Fig. 1) at different levels of the thoracic aorta. Every plane was divided into six segments; 0-point is in the inner curvature of aorta (Fig. 1B) and first segment located anticlockwise. Main parameters under interest were flow displacement (FD), wall shear stress (WSS), regurgitation fraction, maximum velocity and flow, and backward velocity.Results
In the dilated AA group, blood flow was displaced to outer curvature. FD was most prominent in planes 3 and 4 (Table 2). In plane 3, the median FD was 4.5 % in the dilated AA group compared to 2.0 % in the non-dilated AA group (p<0.001). WSS was higher on the lateral side of the aorta where blood flow was displaced, being 1.3-times higher on the side of the aortic wall that was closest to the center of flow as compared to the opposite side (p<0.01). WSS proved to be more circumferential in dilated AAs in comparison to non-dilated AAs. The fraction between circumferential WSS and total WSS (WSSC / WSS) was higher in the dilated AAs when measured from the inner curvature of AA in planes 1–4 and in the whole aortic ring in plane 5 (Table 3). In the dilated AA group, the backward flow fraction to forward flow was increased in planes 3–10 as compared to the non-dilated AA group (median 3.2 %, range 1.5–5.3 % vs. median 0.5 %, range 0.1–0.9 %, p<0.001). The maximum fraction was detected in plane 7 in the middle of the aortic arch, being 5.0 % in the dilated AA group as compared to 1.0 % in the non-dilated AA group (p<0.001). The maximum backward flow velocities were higher in the dilated AA group (37.1±13.5 cm/s) than in the non-dilated AA group (25.7±9.2 cm/s, p<0.01) in planes 1, 5, 6 and 7.Discussion
The present study with TAV patients highlights that flow displacement in the aorta leads to increased WSS to the displaced side. In patients with dilated AAs, the fraction between circumferential and total WSS was higher in the inner curvature of the proximal AA and in the whole ring of the distal aorta when compared to the non-dilated AA group. This indicates that the flow pattern is helical throughout the whole dilated AA. Visual streamline inspection of our data shows that helical flow associates with a dominance of circumferential WSS (Fig. 1 and 2) which is in agreement with the published literature (7). In contrast, axial WSS is dominant in normal laminar flow (7).Conclusion
Aortic flow is displaced in dilated AA compared to non-dilated AA. The flow displacement associates to the increase in WSS on the side of the displacement. This data might be used for the risk stratification of patients with AA dilatation in the future.Acknowledgements
S. Petteri Kauhanen: Personal grant from the will of Oiva Vaittinen and the Rättimäki Cardiovascular SocietyReferences
(1) Markl M, Schnell S, Wu C, Bollache E, Jarvis K, Barker AJ, et al. Advanced flow MRI: emerging techniques and applications. Clin Radiol 2016 Aug;71(8):779-795. (2) Burk J, Blanke P, Stankovic Z, Barker A, Russe M, Geiger J, et al. Evaluation of 3D blood flow patterns and wall shear stress in the normal and dilated thoracic aorta using flow-sensitive 4D CMR. J Cardiovasc Magn Reson 2012 Dec 13;14:84. (3) van Ooij P, Potters WV, Nederveen AJ, Allen BD, Collins J, Carr J, et al. A methodology to detect abnormal relative wall shear stress on the full surface of the thoracic aorta using four-dimensional flow MRI. Magn Reson Med 2015 Mar;73(3):1216-1227. (4) van Ooij P, Markl M, Collins JD, Carr JC, Rigsby C, Bonow RO, et al. Aortic Valve Stenosis Alters Expression of Regional Aortic Wall Shear Stress: New Insights From a 4-Dimensional Flow Magnetic Resonance Imaging Study of 571 Subjects. J Am Heart Assoc 2017 Sep 13,;6(9). (5) Dyverfeldt P, Bissell M, Barker AJ, Bolger AF, Carlhall CJ, Ebbers T, et al. 4D flow cardiovascular magnetic resonance consensus statement. J Cardiovasc Magn Reson 2015 Aug 10;17:5. (6) Roman MJ, Pugh NL, Devereux RB, Eagle KA, Holmes K, LeMaire SA, et al. Aortic Dilatation Associated With Bicuspid Aortic Valve: Relation to Sex, Hemodynamics, and Valve Morphology (the National Heart Lung and Blood Institute-Sponsored National Registry of Genetically Triggered Thoracic Aortic Aneurysms and Cardiovascular Conditions). Am J Cardiol 2017 Oct 01,;120(7):1171-1175. (7) Meierhofer C, Schneider EP, Lyko C, Hutter A, Martinoff S, Markl M, et al. Wall shear stress and flow patterns in the ascending aorta in patients with bicuspid aortic valves differ significantly from tricuspid aortic valves: a prospective study. Eur Heart J Cardiovasc Imaging 2013 Aug;14(8):797-804.Figures
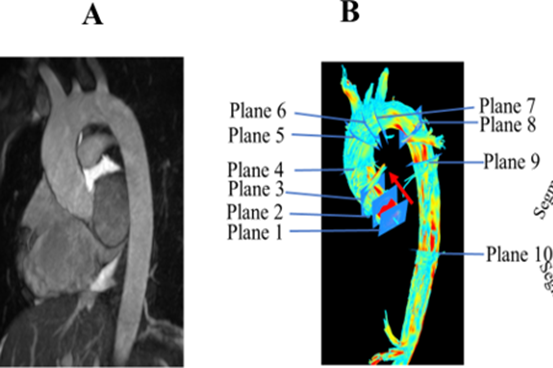
Figure 1. A)
Anatomical view of non-dilated AA in a 23-year-old man by SSFP imaging. The diameter
of the sinus valsalva is 37 mm and the diameter of the tubular plane is 30 mm.
B) An illustration of the 4D flow pattern in a non-dilated aorta. The
streamline blood jet flow pattern is normal (laminar). The positions of the ten
measurement planes are shown. Red arrow shows inner curvature of aorta and
0-point for wall shear stress measurements.
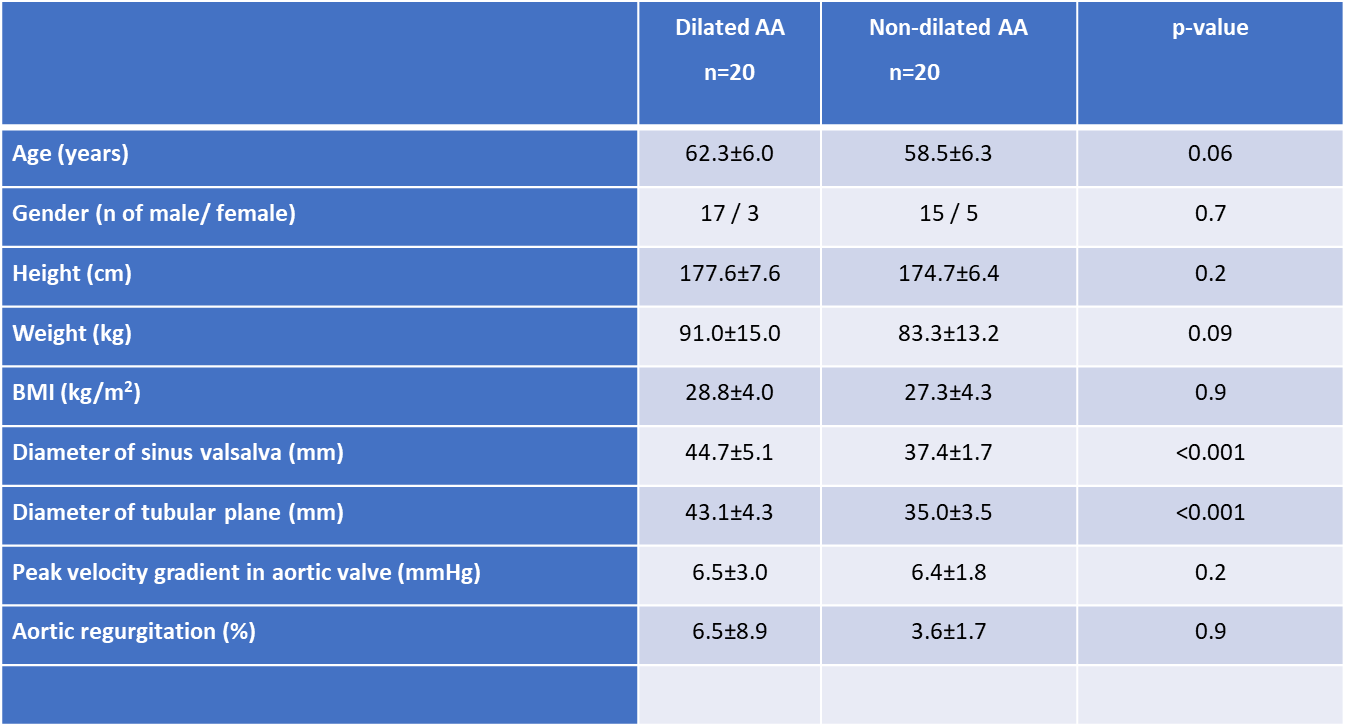
Table 1. Baseline characteristics of the patients. Values of the continuous variables are
mean ± SD.
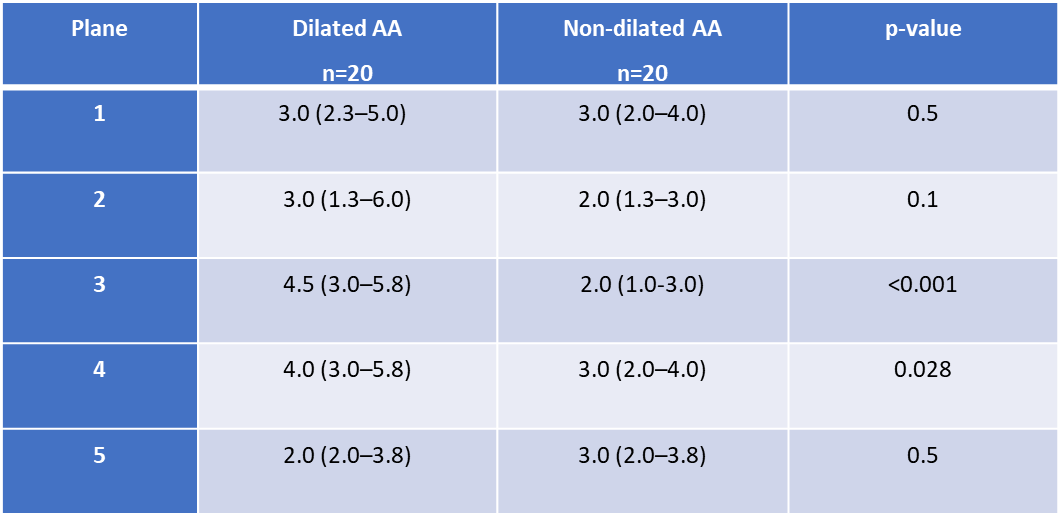
Table 2. Median flow displacement
(FD) values displayed as percentages and ranges for the dilated and the
non-dilated groups. Statistical difference between groups assessed by
Mann-Whitney –test.
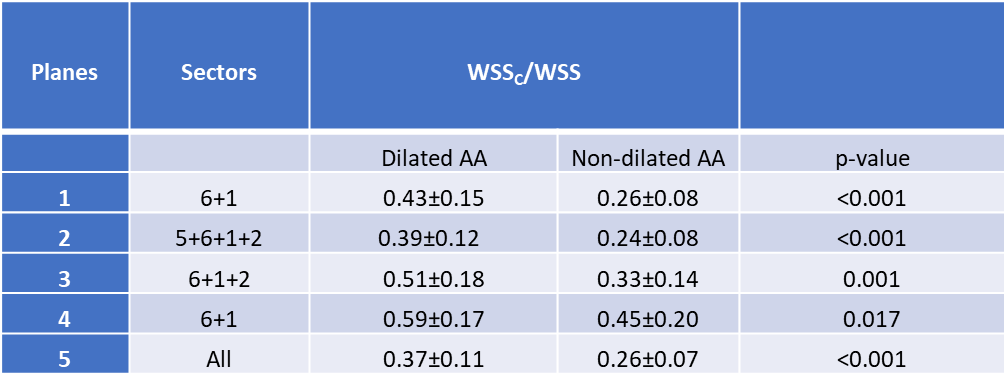
Table 3. Mean values (±SD)
of circumferential and total wall shear stress ratio (WSSC / WSS) in
the dilated AA and the non-dilated AA groups.