1978
Is Right Ventricular Kinetic Energy Correlated with Repaired Tetralogy of Fallot Outcome?1Medical Physics, University of Wisconsin - Madison, Madison, WI, United States, 2Radiology, University of Wisconsin - Madison, Madison, WI, United States
Synopsis
Many patients with repaired Tetralogy of Fallot require additional pulmonary valve replacement surgery later in life. Previous 4D flow MRI studies have suggested that right ventricular kinetic energy may be a useful biomarker in this patient population. In this long-term follow-up study, kinetic energy measurements derived from 4D flow MRI were compared with each patient’s need for pulmonary valve replacement surgery in the next decade. Patients who did not need surgery showed significantly higher stroke volume index normalized by kinetic energy than those who required surgery, suggesting this parameter may have some prognostic value in this application.
Introduction
Tetralogy of Fallot (TOF) is the most common congenital heart disease and accounts for 9-14% of all congenital cardiovascular defects1. Most TOF patients undergo corrective surgery in infancy, but many TOF patients require an additional pulmonary valve replacement (PVR) later in life. The decision-making for this intervention is guided through monitoring of the patient’s right ventricular ejection fraction (RVEF) and RV end diastolic volume index (RV EDVindex). A recent study2, however, has suggested that stroke volume index (SVindex) normalized by right ventricular kinetic energy (KE) as measured with 4D flow MRI, colloquially called RV KE ‘efficiency’ (RV KEE), may be more sensitive to differences in cardiac function between TOF patients and healthy controls than traditional metrics. This ten year follow-up study investigated the potential correlation of RV KE measurements and the eventual need for PVR surgery in a small group of patients with repaired Tetralogy of Fallot (rTOF).Methods
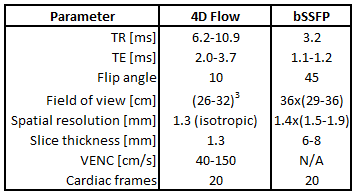
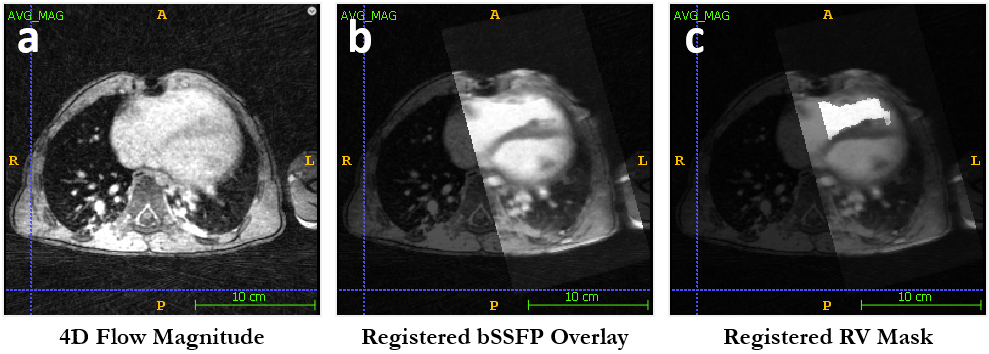
From 2008-2009, nine patients (20.8±13.7 years at time of scanning; 4 male, 5 female) with rTOF underwent cardiac imaging on either a 1.5 T (HDx, GE Healthcare) or 3.0 T (MR750, GE Healthcare) MRI scanner, depending on clinical availability. 4D flow imaging was performed with a radially undersampled phase contrast sequence (PC VIPR3,4) and 2D cine bSSFP images were acquired in a short axis orientation for whole heart coverage. The scan parameters for these sequences are presented in Figure 1. Using Segment5 (http://segment.heiberg.se), RV endocardial borders were contoured for all cardiac frames and slices in the bSSFP images. RV EDVindex and EF was calculated for each patient using these endocardial contours. Using the method described by Gupta et al.6, the short-axis bSSFP images were registered to the 4D flow imaging volume to apply the segmented RV mask from bSSFP to the 4D flow data, as shown in Figure 2. RV KE and RV KEE was calculated for each time frame. A medical record follow-up was performed on all patients to identify who required PVR surgery in the last decade. T-tests were used to determine any significant differences in RV EDVindex, RVEF, peak systolic RV KE, and peak systolic RV KEE at the time of the initial MRI scan between patients who did and did not eventually require additional surgery.Results
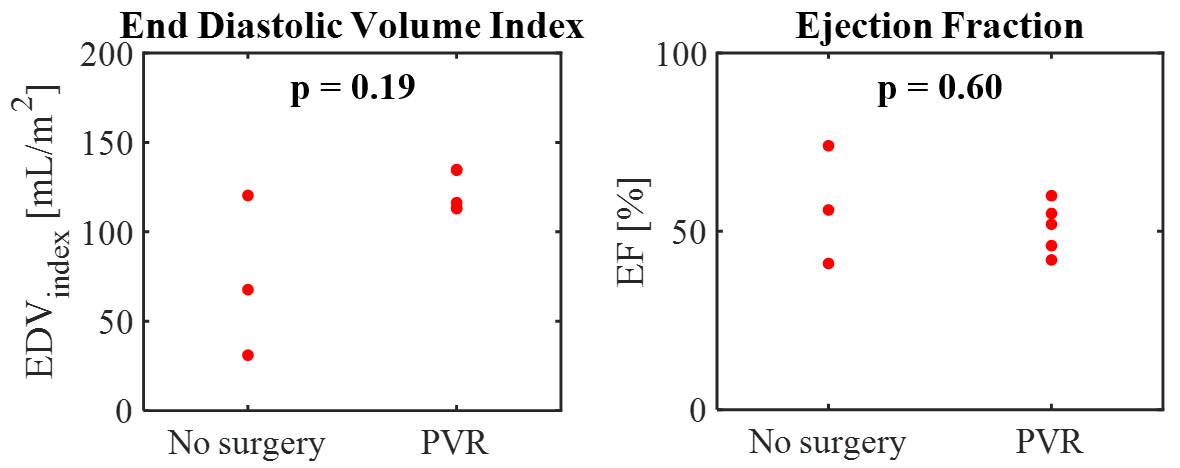
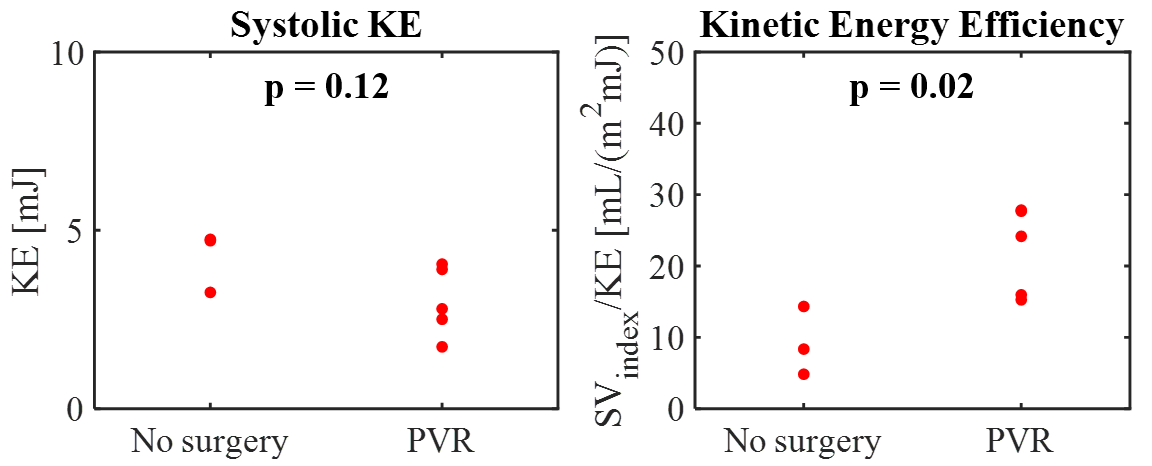
The bSSFP images could not be registered to the 4D flow images in one patient due to differences in respiratory state between acquisitions, prohibiting 4D flow KE analysis. Figure 3 shows RV EDVindex and RVEF distributions for both patient groups. These metrics showed no significant differences between groups: RV EDVindex was 73.0±44.9 mL/m2 in patients with no PVR surgery and 122.4±11.3 mL/m2 in those requiring PVR (p=0.19) while RVEF was 57±17% and 51±7% respectively in these groups (p=0.6). Figure 4 shows RV KE and RV KEE distributions during peak-systole for each group. While systolic RV KE also showed non-significant differences (No surgery: 4.2±0.8 mJ, PVR: 3.0±1.0 mJ, p=0.12), indexed systolic RV KEE demonstrated significant differences between the two patient groups (No surgery: 9.2±4.8 mL/(m2mJ), PVR: 22.2±6.2 mL/(m2mJ), p=0.02).Discussion
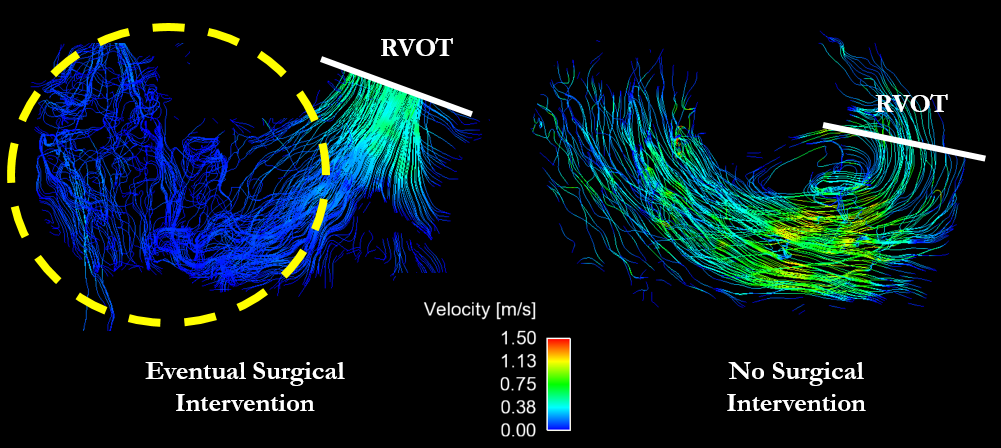
In this limited sample size, SVindex normalized by RV KE, or RV KEE, demonstrated greater statistical differences between patients with rTOF who would eventually require PVR and those who would not than conventional metrics such as RV EDVindex and RVEF. This result, coupled with that from previous TOF studies2, suggest KE may hold prognostic and diagnostic value in this population. Counterintuitively, the TOF patients who eventually required surgery were those that demonstrated higher RV KEE. Streamline visualizations in representative patients from both groups (Figure 5) helped elucidate this result. Subjects requiring no additional surgery demonstrated laminar streamlines traversing the entire RV during systolic ejection whereas patients requiring eventual PVR featured slow, unstructured flow in the region of the RV distal from the pulmonary valve. This resulted in lower KE and higher KEE in these subjects, even though they demonstrated abnormal flow patterns. This may suggest altered myocardial contraction and highlights the limitations of KEE as a standalone metric. Future work will follow-up on more subjects to increase the sample size of this work and expand this analysis to include local myocardial strain assessment.Conclusion
Initial analysis from this long-term follow-up study in patients with rTOF showed significant differences in systolic RV KEE between patients who required PVR in the ten years following their initial scan and those who did not. Significant differences were not observed in clinical parameters such as EDVindex and EF, suggesting KEE could be a useful prognostic biomarker in this patient population.Acknowledgements
No acknowledgement found.References
1. Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart disease and stroke statistics-2010 update: a report from the American Heart Association. Circulation. 2010; 121.
2. Jeong D, Anagnostopoulos PV, Roldan-Alzate A, et al. Ventricular kinetic energy may provide a novel noninvasive way to assess ventricular performance in patients with repaired Tetralogy of Fallot. J Thorac Cardiovasc Surg. 2015; 149(5): 1339-1347.
3. Gu T, Korosec FR, Block WF, Fain SB, et al. PC VIPR: a high-speed 3D phase-contrast method for flow quantification and high-resolution angiography. AJNR. 2005; 26(4): 743-749.
4. Johnson KM, Lum DP, Turski PA, Block WF, et al. Improved 3D phase contrast MRI with off-resonance corrected dual echo VIPR. MRM. 2008; 60(6): 1329-1336.
5. Heiberg E, Sjogren J, Ugander M, et al. Design and Validation of Segment – a Freely Available Software for Cardiovascular Image Analysis. BMC Medical Imaging. 2010; 10(1).
6. Gupta V, Bustamante M, Fredriksson A, et al. Improving Left Ventricular Segmentation in Four-Dimensional Flow MRI Using Intramodality Image Registration for Cardiac Blood Flow Analysis. MRM. 2018; 79(1): 554-560.
Figures