1977
Left and Right Heart Ventricular-Vascular Coupling in Pulmonary Venous Hypertension1Radiology, Northwestern University, Chicago, IL, United States, 2Pulmonary and Critical Care, Northwestern University, Chicago, IL, United States, 3Cardiology, Northwestern University, Chicago, IL, United States
Synopsis
Pulmonary Venous hypertension (PVH) is a life-threatening disease with a complex etiology that involves both the left and right heart. However, the mechanism of left heart dysfunction as a precursor to changes in right heart hemodynamics and dysfunction remains unclear. Here, we assessed the complex functional-hemodynamic coupling between the left and right heart and pulmonary arteries. We investigated the association of LV and RV function with advanced 4D Flow MRI hemodynamic metrics of volumetric viscous energy loss, kinetic energy and vorticity in the right heart and pulmonary arteries in PVH patients.
Purpose:
Pulmonary Venous hypertension (PVH) is a life-threatening disease with a complex etiology that involves both the left and right heart. While PVH is manifested in an overload in hemodynamic pulmonary arterial pressure, it originates as a result of left heart dysfunction. However, the mechanism of left heart dysfunction as a precursor to changes in right heart/pulmonary hemodynamics and dysfunction remains unclear. Hence, a better understanding of the complex functional-hemodynamic coupling between the left and right heart/pulmonary could enable insights into early noninvasive markers of PH disease onset and progression. The aims of this study were to 1) assess association of LV and RV function with advanced 4D Flow MRI hemodynamic metrics of volumetric viscous energy loss (EL), vorticity and kinetic energy (KE) in the right ventricle (RV) and pulmonary arteries (main pulmonary artery (MPA), left (LPA) and right pulmonary arteries (RPA)) in PVH patients; and to 2) compare EL, KE and vorticity hemodynamics between PVH patients with normal vs. impaired systolic function.Methods:
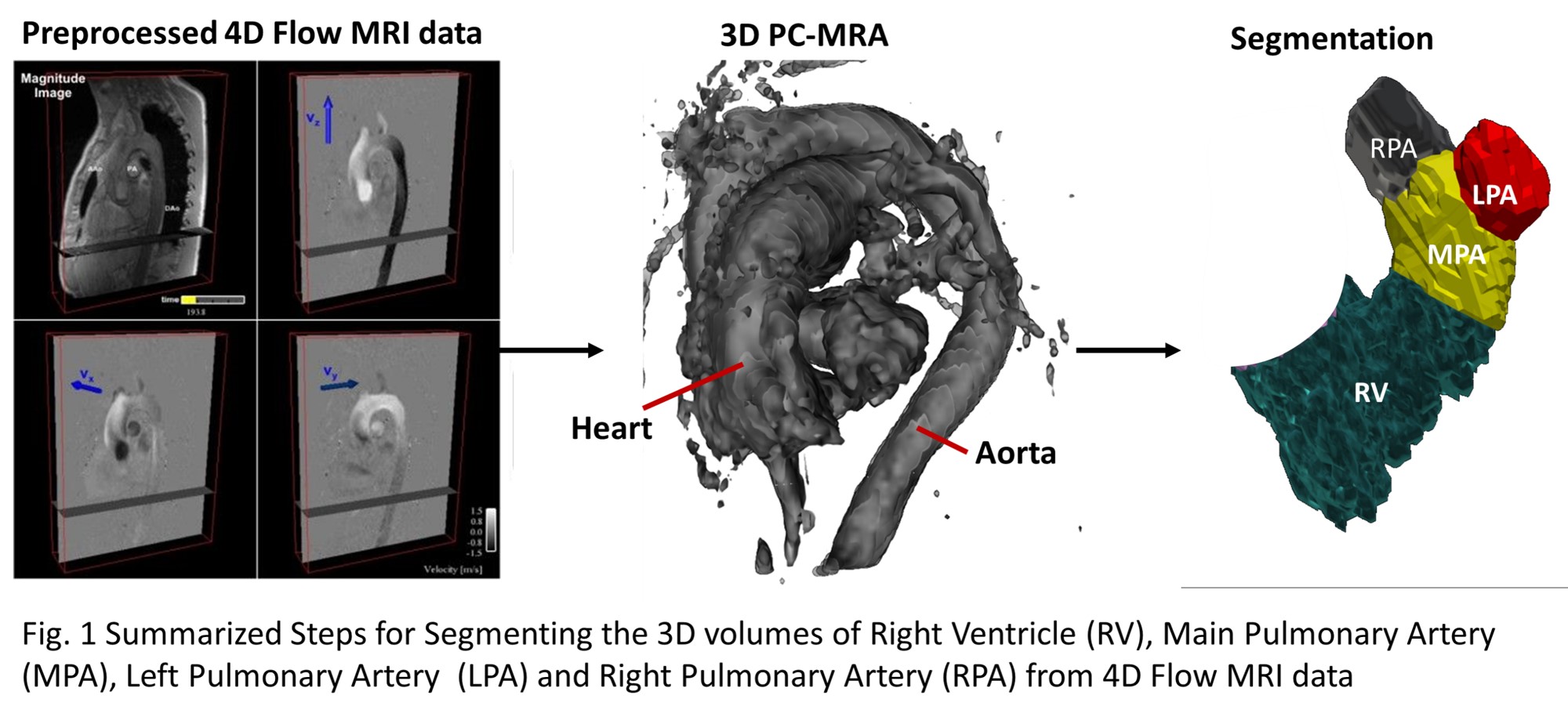
A total of 16 PVH patients (age: 60±14 years, 9 female) were prospectively included from an ongoing IRB-approved study (Table1). PVH patients were diagnosed according to [1]. Whole-heart 4D Flow MRI was performed at 1.5T (Siemens) during free breathing with respiratory navigator gating (spatial resolution = (2.4-2.7)×(2.4-2.7)×(3-3.2)mm3, temporal resolution = 33–43ms, venc = 100-200 cm/s). Data analysis (Fig. 1) included the calculation of a 4D flow MRI-derived 3D PC angiogram (PCMRA) for the 3D segmentation of the RV, MPA, LPA, and RPA. Per 3D segment, systolic peak of volumetric Kinetic energy (KEpeak-systole), viscous energy loss rate (ELpeak-systole) and vorticity (Vorticity-volpeak-systole) were computed (Fig.2) [2, 3]. All parameters were normalized by volume. To assess the left and right ventricular function, standard cine short axis MR images were manually segmented and used to compute left and right ventricular ejection fraction (LVEF, RVEF) as well as stroke volumes (LVSV, RVSV). Patients were then divided into two groups based on systolic RV function: (impaired systolic function: RVEF<=40% and normal systolic function RVEF>=50%). Similarly, patients were divided into another two groups based on systolic LV function: (impaired systolic function: LVEF<=40% and normal systolic function LVEF>=50%). Spearman correlation was used to test associations and Wilcoxon’s rank sum test was used for statistical comparisons.Results:
Table2. provides detailed results of functional correlation to 4D Flow hemodynamics. Strongest LV and RV functional associations were found with LPA hemodynamics: (ELpeak_systole vs RVSV: rho=0.9, p<0.0001; ELpeak_systole vs RVEF: rho=0.67, p=0.005). Importantly, LPA ELpeak_systole showed significant positive correlation with LVEF (rho=0.67, p=0.005) and LVSV (rho=0.62, p=0.01). LPA Vorticity-volpeak_systole vs. RVSV: 0.86, p<0.0001; Vorticity-volpeak_systole vs. RVEF: rho=0.66, p=0.006). No significant correlations were found with LPA KEpeak-systole. For the RPA, significant hemodynamic correlations were found only with RVSV: (ELpeak_systole: rho=0.63, p=0.01, Vorticity-volpeak_systole: rho=0.67, p=0.005, KEpeak-systole: rho=0.64, p=0.008). Likewise, for the MPA, only RVSV showed significant correlation with hemodynamics (ELpeak_systole: rho=0.60, p=0.01, Vorticity-volpeak_systole: rho=0.71, p=0.005, KEpeak-systole: rho=0.65, p=0.007). In the RV, the only significant correlation was found between RVEF and Vorticity-volpeak_systole: rho=0.75, p=0.001.
Table.1 shows the global function of LV and RV. Systolic RV function groups were (N=7 with RVEF<40%, N=8 with RVEF>50%; age: 57±16 years vs.62±13, p=0.71). Dividing PVH patients into two groups based on LVEF resulted in (N=6 with LVEF<40%, N=9 with LVEF>50%; age: 64±17 years vs.60±12, p=0.34). Notably, Fig.3 shows that LPA hemodynamics presented significant differences between the group of PVH patients with impaired RV systolic function compared to the PVH group with normal RV systolic function. The impaired group showed significantly reduced ELpeak_systole and Vorticity-volpeak_systole (p=0.01). Similarly, LPA showed significantly reduced ELpeak_systole and Vorticity-volpeak_systole in the PVH group with impaired systolic LV function as compared to the PVH group with normal LV systolic function (p=0.02). Moreover, the RV showed significantly reduced Vorticity-volpeak_systole in the group with impaired RV function.
Discussion and conclusions:
The findings of this study indicate a functional coupling of the left and right ventricular systolic function with the right heart ventricular and the pulmonary artery hemodynamics in PVH patients. Such coupling appeared strongest for the LPA which demonstrated significant associations with both LV and RV systolic function. These findings from our pilot study suggest that LPA hemodynamics might be most sensitive to functional changes in PVH patients. Future studies with large PVH patient cohorts are warranted to further study the impact of functional-hemodynamic coupling on PVH patient outcome.Acknowledgements
No acknowledgement found.References
[1] Freed, Benjamin H. et al. JACC. Cardiovascular imaging 9.6 (2016): 715–732.
[2] Elbaz MSM et al. Magnetic resonance in medicine77, no. 2 (2017): 794-805
[3] Kamphuis V., Elbaz MSM, et al. (2018). European Heart Journal-Cardiovascular Imaging.
Figures