1968
An application of the myocardial strain analysis method based on the deformation registration algorithm (DRA) in heart transplantation1Department of Radiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, 2Department of Ultrasound, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, 3MR Collaboration, Siemens Healthcare Ltd., Shanghai, China., Shanghai, China
Synopsis
With the development of cardiac magnetic resonance(CMR), there have been various methods to quantify myocardium. As a novel method, deformation registration algorithm (DRA) has been confirmed in many cardiac diseases. In this article, we use this method to analyze the wall deformation of orthotopic heart transplantation(HTx). We found that though left ventricular ejection fraction (LVEF) have no significant difference between the HTx patients and the healthy volunteers, the left ventricular (LV) peak longitudinal strain (LV Ell) and LV peak systolic longitudinal strain rate have significant decrease in HTx patients, indicating that the ventricular deformation is more sensitive than LVEF in response to the myocardial diseases.
Introduction
Over the decades, many papers on left ventricular (LV) wall deformation had reported that abnormal deformation is associated with the prognosis of patients with coronary or other heart diseases, and several papers1,2 reported that this deformation abnormality is associated with higher risks of needing the clinical treatment without overt decrease of the LVEF. Myocardial strain based on the deformation registration algorithm (DRA) proved to be a sensitive tool of measuring the abnormal deformation of the heart3. Nowadays there has few research applying the DRA to HTx patients. Our aim is to investigate whether LV wall deformation has difference between the HTx patients and the healthy population with LVEF in the normal range.Method
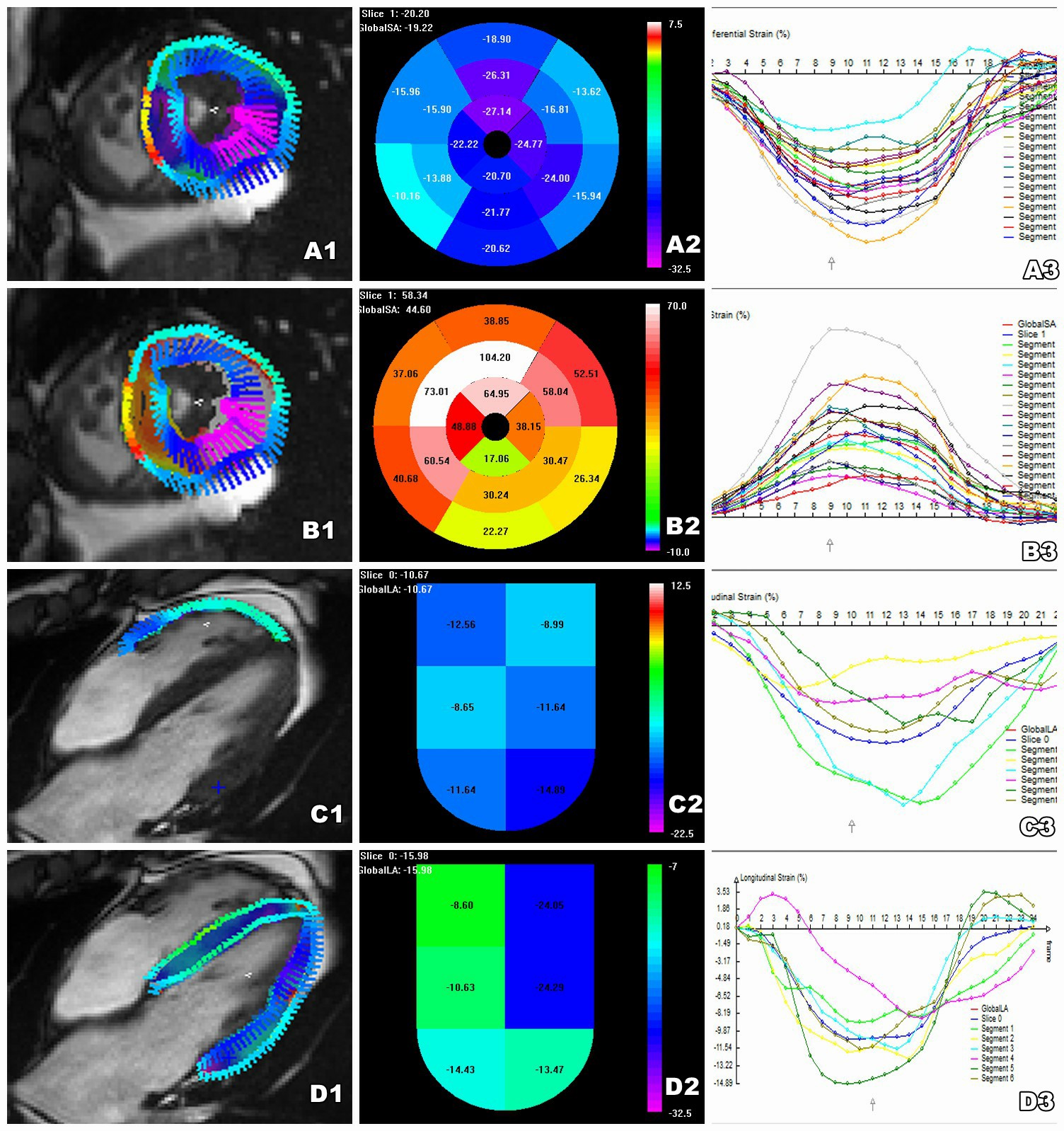
About 24 consecutive cardiac transplant recipients in their routine clinical protocol(6 female; 48±11.5 years) at a median of 2.8 years (0.8–14 years) after HTx and 15 healthy volunteers (6 female; 40±12.8 years) were enrolled in the study from August to October in 2018 in Wuhan Union Hospital, Wuhan, China. The exclusion criteria included chronic atrial fibrillation, current confirmed or clinically indicated significant acute rejection, and contraindications to cardiovascular magnetic resonance (CMR) imaging. For each participant, balanced steady-state free precession (bSSFP) sequences were used to acquire cardiac cine images about long-axis and short-axis. A 1.5T MR scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany) was used with an 18-channel phased array body coil combined with a spine coil (12 channels used) during a breath-hold of 10 to 15 seconds. LVEF, LV end-diastolic volume (LVEDS) and LV end-systolic volume (LVESV) were calculated between the HTx patients and the volunteers. The global LV and the right ventricular free wall (RV FW) peak longitudinal strain (Ell), LV global peak radial strain (Err) and LV global peak circumferential strain (Ecc) and their respective systolic strain rates were analyzed using a prototype DRA based software (TrufiStrain, version 2.0, Siemens Healthcare, Erlangen, Germany), as shown in Fig.1. All of the parameters were derived from the full ventricle wall, containing endocardium, myocardium and epicardium.Results
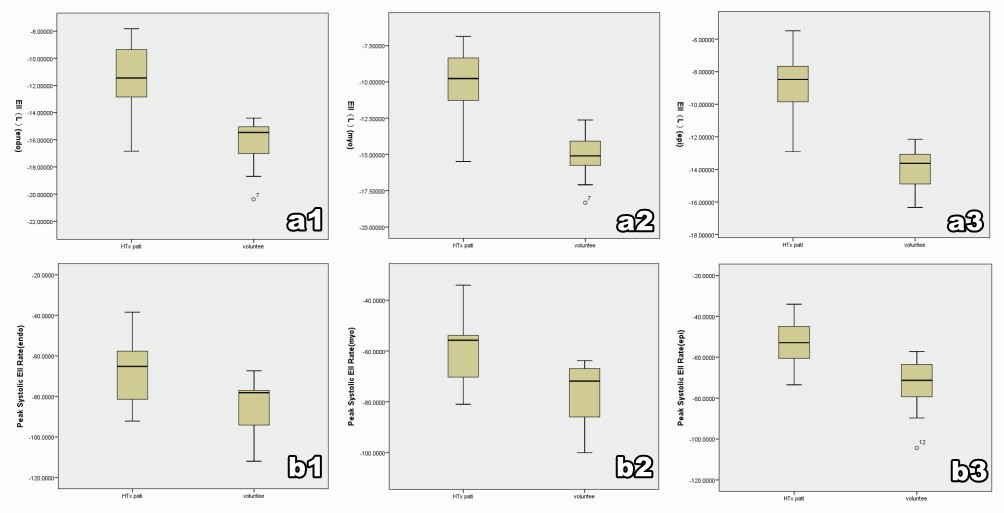
We find that LVEF, LVEDV and LVESV have no significant difference between the HTx patients and the healthy volunteers. We also find the gradual decrease from endocardium to epicardium in LV Ell and LV peak systolic longitudinal strain rate for both the HTx patients and the volunteers. A paper4 found this similar change in healthy populations. However, the LV Ell have significant decrease in HTx patients compared with the healthy volunteers in full ventricular wall (endo: -11.32%±2.48% vs -16.32%±1.68%; P<0.001; myo: -10.03%±2.13% vs -14.95±1.98%; P<0.001, epi: -8.85%±1.81% vs -13.89%±1.29%; P<0.001), and the LV peak systolic longitudinal strain rate also have significant decrease in HTx patients compared to the healthy volunteers (endo: -67.73s-1±15.47s-1 vs -84.32s-1±12.25s-1; P=0.001; myo: -59.40s-1±13.67s-1 vs -76.65s-1±11.39s-1; P<0.001; epi: -14.78s-1±2.85s-1 vs -16.55s-1±2.22s-1; P<0.001). The results are shown in Fig. 2. The LV Err, LV Ecc, RV FW-Ell and their peak systolic strain rate have no statistically signification between the HTx patients and the healthy volunteers.Discussion
Myocardial strain analysis based on the CMR cine images is a non-invasive quantification method without adding additional clinical examination time. Moreover, DRA is a reliable and robust analysis tool for quantifying the segmental myocardial strain5. A paper showed excellent accuracy using DRA for the detection of myocardial strain differences between hypertrophic cardiomyopathy (HCM) and healthy subjects compared with the feature tracking (FT) method or speckle tracking echocardiography (STE), which might due to DRA’s superior reproducibility5. Previous studies have shown that LV wall deformation occurred at an early stage when EF is still within the normal range in HCM patients6. According to our results, we find the significant decrease in LV Ell and LV peak systolic longitudinal strain rate among HTx patients compared with the healthy volunteers. This indicates that the variation of ventricular wall deformation is earlier than the decrease of the LVEF in response to myocardial diseases.Conclusion
LV Ell and LV peak systolic longitudinal strain rate may be a sensitive biomarker for the early deformation change of the ventricular wall in HTx patients. Decreased LV Ell and LV peak systolic longitudinal strain rate maybe have a relationship with the prognosis of the HTx patients.Acknowledgements
No acknowledgement found.References
1.Cicala S, de Simone G, Roman MJ, et al. Prevalence and prognostic significance of wall-motion abnormalities in adults without clinically recognized cardiovascular disease: the Strong Heart Study. Circulation. 2007; 116(2):1432):143PubMed: 17576870 .2.Tang X, Yu S, Yu Y, et al. Left ventricular myocardial strain in ventricular arrhythmia without structural heart disease using cardiac magnetic resonance. American Journal of Translational Research, 2017, 9(6):3006.3.Jolly M P, Guetter C, Lu X, et al. Automatic Segmentation of the Myocardium in Cine MR Images Using Deformable Registration Statistical Atlases and Computational Models of the Heart. Imaging and Modelling Challenges. Springer Berlin Heidelberg, 2012:98-108.4.Liu H, Yang D, Wan K, et al. Distribution pattern of left-ventricular myocardial strain analyzed by a cine MRI based deformation registration algorithm in healthy Chinese volunteers. Scientific Reports, 2017, 7:45314.5.Wang J, Li W, Sun J, et al. Improved segmental myocardial strain reproducibility using deformable registration algorithms compared with feature tracking cardiac MRI and speckle tracking echocardiography. Journal of Magnetic Resonance Imaging Jmri, 2017.6.Mcleod C J, Bos JMTheis J L. Histologic characterization of hypertrophic cardiomyopathy with and without myofilament mutations. American Heart Journal, 2009, 158(5):799-805.Figures