1951
Phase contrast coronary blood velocity mapping with both high temporal and spatial resolution using Golden Angle rotated Spiral k-t Sparse Parallel imaging (GASSP)1Department of Biomedical Engineering, The Johns Hopkins University School of Medicine, Baltimore, MD, United States, 2Division of Cardiology, Department of Medicine, The Johns Hopkins University School of Medicine, Baltimore, MD, United States, 3Russell H. Morgan Department of Radiology and Radiological Science, The Johns Hopkins University School of Medicine, Baltimore, MD, United States
Synopsis
Coronary phase contrast MRI for accurate measurement of coronary blood flow requires high spatial resolution due to the small vessel size, and high temporal resolution due to cardiac motion, especially of the right coronary artery (RCA). This study uses golden angle rotated spiral k-t sparse parallel imaging (GASSP) to accelerate the acquisition to achieve both high spatial and high temporal resolution in a breath-hold. GASSP was validated in the stationary popliteal artery (knee) and then implemented in the RCA. GASSP achieved high image quality throughout the cardiac cycle and popliteal peak velocity and mean-square error compared favorably to gold standard.
INTRODUCTION
Coronary phase contrast (PC) MRI can be used to diagnose coronary artery disease1, and variants of the technique have recently been explored to measure pressure gradients across stenosis2 and coronary endothelial function3. Current breath-held techniques focus on either measuring accurate and reproducible coronary peak velocity, which requires high spatial resolution ($$$\Delta$$$x=0.8mm in4) but may suffer from motion blurring, or assessing the temporal patterns of coronary blood flow through the cardiac cycle, which requires high temporal resolution ($$$\Delta$$$t<20ms in5). This study aims to achieve phase contrast coronary MRI with both high spatial and high temporal resolution to accurately measure the coronary flow velocity throughout the cardiac cycle by accelerating the acquisition with golden angle rotated spiral k-t sparse parallel imaging (GASSP).
To validate the proposed GASSP PC method, a 5-minute high resolution Cartesian acquisition was performed in the (non-moving) popliteal artery. For the RCA, two previously validated breath-hold acquisitions4,5 were performed, one with high spatial resolution to validate peak velocity measurements4 and one with high temporal resolution to validate the temporal pattern of blood flow5.
METHODS
IRB approved studies were performed of the popliteal artery in 3 and the right coronary artery (RCA) in 4 healthy subjects. Popliteal arteries were scanned twice. All scans were performed on a 3T scanner (Achieva, Philips Healthcare). A two-dimensional gradient echo sequence was used with a spiral readout trajectory, spectral-spatial excitation, and two-sided velocity encoding in slice direction, applying a venc of 100cm/s and 35cm/s for popliteal and RCA, respectively. The imaging slice was oriented orthogonal to arteries.
High Spatial Resolution Protocol4: 11 spiral arms are acquired with positive and negative flow encoding interleaved every other heartbeat leading to 22 heartbeats. High spatial resolution of $$$\Delta$$$x=0.8mm leads to long spiral readout of ~33ms and long repetition time (TR)=40ms. The acquisition is ECG-triggered and the number of cardiac phases depends on the heart rate. Parameters: field of view (FOV)=250x250mm2, echo time TE=2.9ms for popliteal and TE=3.5ms for RCA.
High Temporal Resolution Protocol5: 11 spiral arms are acquired with positive and negative flow encoding interleaved every other heartbeat leading to 22 heartbeats. High temporal resolution of $$$\Delta$$$t=20ms requires short readout duration of 13ms but worsens the spatial resolution to $$$\Delta$$$x=1.4mm. The acquisition is retrospectively ECG-gated to 50 cardiac phases. Parameters: FOV =350x350mm2, TR/TE=19.2/2.6ms for popliteal and TR/TE=19.8/3.2ms for RCA.
GASSP Protocol: 500 Spiral arms are acquired for each flow encoding. Spiral arms are rotated by the golden angle (137.508°)6 after both flow encodings are acquired leading to a ~20s scan (TR=20ms). Arms are retrospectively binned into 50 cardiac phases according to their ECG-time stamps with different flow encodings sorted separately. Binned data will be incoherently under-sampled and compressed sensing7-9 type of reconstruction is performed to minimize the combination of parallel-imaging data consistency and temporal total-variation based sparsity constraints. Parameters: FOV = 350x350mm2, $$$\Delta$$$x=0.8mm, TR/TE=19.3/2.6ms for popliteal and TR/TE=19.8/3.2ms for RCA.
High Resolution Cartesian Protocol: The 5-minute Cartesian acquisition is only used in popliteal scans. Parameter: FOV=200x200mm2, $$$\Delta$$$x=0.4mm, TR/TE=5.4/2.8ms, retrospective ECG gated with an acquired temporal resolution of $$$\Delta$$$t=5.4ms.
Data Analysis: Flow-compensated images were calculated by combining positive and negative flow encoded images with a pixel-wise geometric mean and were used to deblur spiral data10 and for vessel segmentation. Popliteal arteries were segmented automatically by full-width-half-maximum threshold. RCA ROIs were circles manually placed on the vessel. We calculated mean velocity and flow (mean velocity $$$\times$$$ area ), peak systolic and peak diastolic values and mean-square-error (MSE):$$$\frac1N||x-x_{ref.}||_2^2$$$, with $$$N$$$ cardiac phases, flow curve $$$x$$$, and $$$x_{ref.}$$$ interpolated from Cartesian curve.
RESULTS
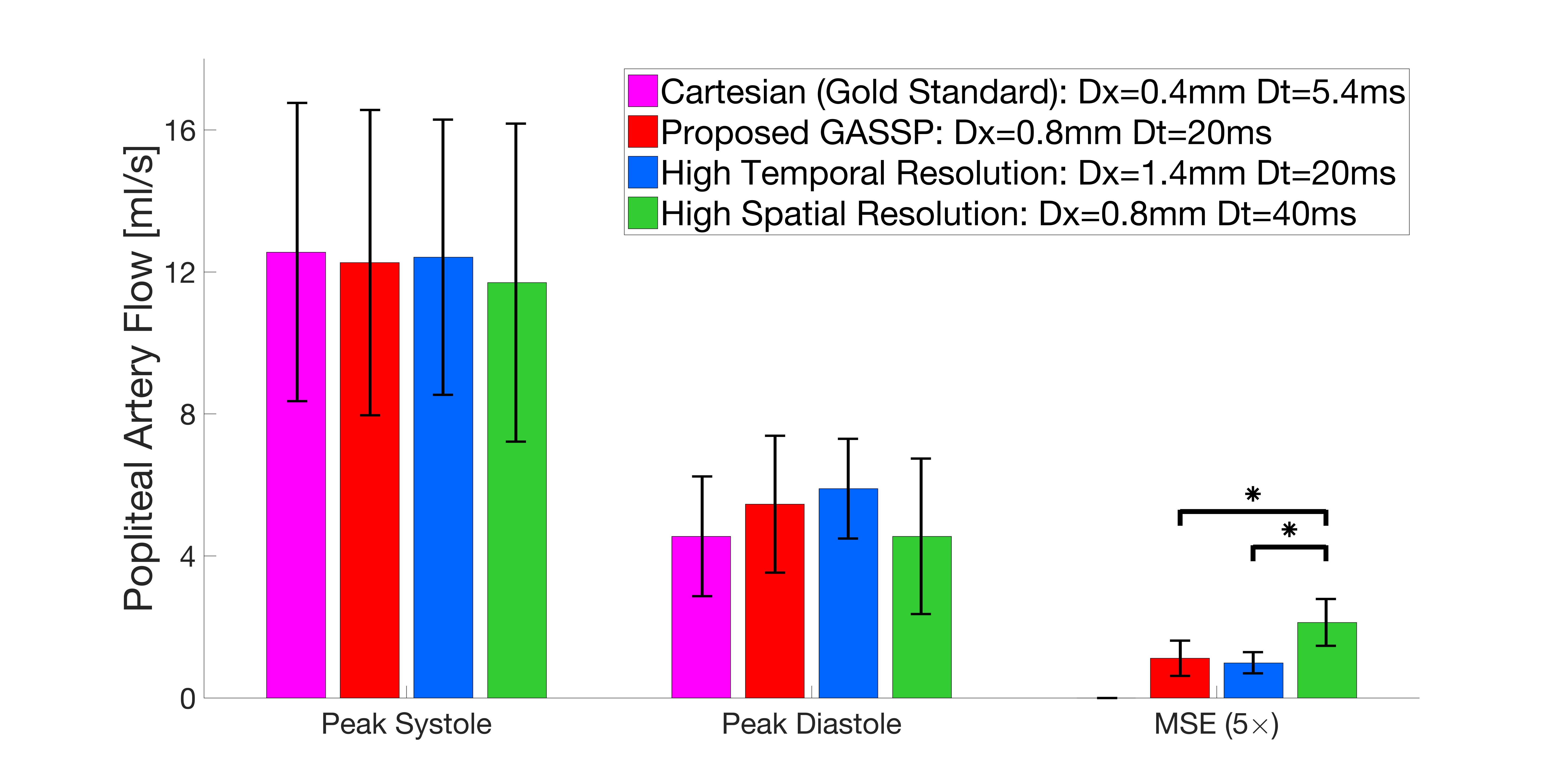
Figure 1 shows representative flow curves of a popliteal artery acquired with the different protocols. The flow curves from the different protocols agree well despite a small temporal shift compared to the reference Cartesian acquisition. Figure 2 shows peak systolic, peak diastolic, and MSE of popliteal blood flow. Peak flow agree well for all methods and MSE is reduced for GASSP and High Temporal compared to High Spatial protocol. Figure 3 shows magnitude and velocity CINE images acquired with the proposed GASSP sequence from all 4 RCA subjects and high image quality is observed throughout the cardiac cycle. Figure 4 shows good agreement of mean coronary blood velocity acquired with the 3 methods in one subject.DISCUSSION AND CONCLUSION
The proposed 20-s GASSP coronary blood flow method with 0.8mm spatial resolution and 20ms temporal resolution agrees well with a 5-minute reference acquisition in non-moving popliteal arteries, and offers excellent image quality throughout the cardiac cycle in the RCA. Quantitative velocity values in the RCA are promising but need to be performed in more subjects and improved vessel segmentation.
Acknowledgements
Work supported by NIH HL120905, HL125059, HL61912 and AHA 17SDG33671007.References
1. Ofili EO, Labovitz AJ, Kern MJ. Coronary flow velocity dynamics in normal and diseased arteries. Am J Cardiol. 1993;71:3D–9D
2. Deng, Z. , Fan, Z. , Lee, S. , Nguyen, C. , Xie, Y. , Pang, J. , Bi, X. , Yang, Q. , Choi, B. , Kim, J. , Berman, D. , Chang, H. and Li, D. (2017), Noninvasive measurement of pressure gradient across a coronary stenosis using phase contrast (PC)‐MRI: A feasibility study. Magn. Reson. Med, 77: 529-537.
3. Hays AG, Hirsch GA, Kelle S, Gerstenblith G, Weiss RG, Stuber M. Noninvasive visualization of coronary artery endothelial function in healthy subjects and in patients with coronary artery disease. J Am Coll Cardiol. 2010;56:1657–1665.
4. Brandts A, Roes SD, Doornbos J, Weiss RG, de Roos A, Stuber M, Westenberg JJM. Right coronary artery flow velocity and volume assessment with spiral K-space sampled breathhold velocity-encoded MRI at 3 tesla: Accuracy and reproducibility. J Magn Reson Imaging. 2010;31:1215–1223.
5. Keegan J, Raphael CE, Parker K, Simpson RM, Strain S, de Silva R, Di Mario C, Collinson J, Stables RH, Wage R, Drivas P, Sugathapala M, Prasad SK, Firmin DN. Validation of high temporal resolution spiral phase velocity mapping of temporal patterns of left and right coronary artery blood flow against Doppler guidewire. J Cardiovasc Magn Reson [Internet]. 2015 [cited 2018 Mar 2];17. Available from: http://jcmr-online.com/content/17/1/85
6. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An optimal radial profile order based on the Golden Ratio for time-resolved MRI. IEEE Trans Med Imaging. 2007;26:68–76.
7. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn Reson Med. 2007;58:1182–1195.
8. Gamper U, Boesiger P, Kozerke S. Compressed sensing in dynamic MRI. Magn Reson Med. 2008;59:365–373.
9. Feng L, Srichai MB, Lim RP, Harrison A, King W, Adluru G, Dibella EVR, Sodickson DK, Otazo R, Kim D. Highly accelerated real-time cardiac cine MRI using k-t SPARSE-SENSE. Magn Reson Med. 2013;70:64–74.
10. Noll DC, Pauly JM, Meyer CH, Nishimura DG, Macovski A. Deblurring for non-2D Fourier transform magnetic resonance imaging. Magn Reson Med. 1992;25:319–333.
Figures